
記住我





In 2021, 33 529 (95%UI 27 769 − 41 395) female deaths were estimated in Mexico due to CKD. Between 1990 and 2021, the number of deaths from CKD women significantly increased by 348% (95% UI 277–437) from 7 484 (95%UI 7 170-7 886) in 1990. The leading causes of female CKD deaths in 2021 were OTH and T2D, each accounting for over 8 000 deaths. Additionally, the number of deaths rose significantly across all CKD sub-causes. The highest growth was seen in T1D-related CKD (395%; 95%UI 280–579), followed by AH (366%; 95%UI 298–454), T2D (351%; 95%UI 286–426), OTH (337%; 95%UI 257–442) and GN (331%; 95%UI 244–449) (data not shown).
The ASR mortality, ASR-DALYs, ASR-YLLs, and ASR-YLDs due to CKD in women are also shown in Table 1. The female ASR mortality due to CKD (per 100 000 inhabitants) increased from 40.4 deaths (95%UI 38.2–43.0) in 1990 to 50.9 (95%UI 42.4–62.3) in 2021 (a significant change of 26.1%; 95%UI 7.2–48.4). Female ASR mortality due to CKD increased for GN, OTH, and T1D between 1990 and 2021. T1D had the highest relative increase (82.2%; 95%UI 40.9-145.4), followed by GN (46.8%; 95%UI 18.8–86.1). In 2021, the highest ASR mortality was found in T2D (12.5; 95%UI 9.8–16), OTH (12.4; 95%UI 9.2–16.5) and AH (12.3; 95%UI 9.4–15.6), with the lowest rate due to T1D (2.4; 95%UI 1.5–3.7). ASR-DALYs due to CKD per 100 000 inhabitants increased 44.7%, from 937.9 (95%UI 893.7–988.0) in 1990 to 1357.1 (95%UI 1112.5, 1708.5) in 2021. Between 1990 and 2021, the female ASR-DALYs due to CKD increased significantly for all sub-causes, especially for T1D, with a rise of 75.5%. In 2021, OTH and GN accounted for 27.5% and 26.3% of the total ASR-DALYs, respectively, while T1D contributed 6.5% to the total ASR-DALYs among women. In 2021, 91% of the female ASR-DALYs due to CKD were attributable to YLLs, while YLDs accounted for only 9%. There was a significant increase of 50.3% in the female ASR-YLLs due to CKD between 1990 and 2021, from 820.7 (95% UI 792-855.7) to 1233.6 (95% UI 1001, 1580.3), respectively. The ASR-YLDs due to CKD had a non-significant increase of 5.4% between 1990 and 2021, from 117.2 (95% UI 83.6–152.0) to 123.5 (95% UI 87.7, 160.1). There was a statistically significant increase in the ASR-YLLs across all CKD sub-causes, while GN was the only CKD sub-cause with a considerable increase in the ASR-YLDs.
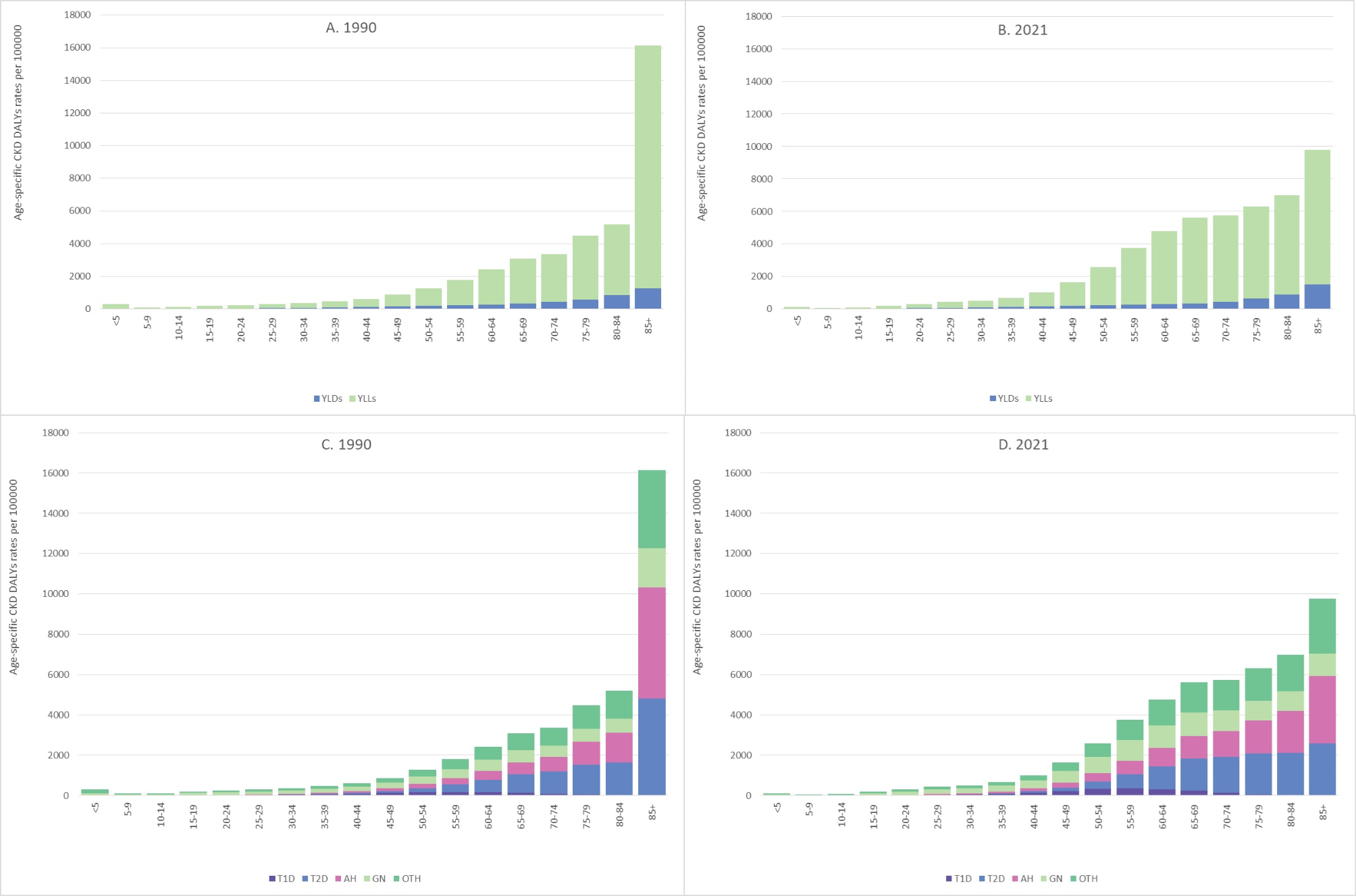
Table 1 Age-standardized rates of disability-adjusted life-years for females due to chronic kidney disease by sub-causes. Mexico, 1990 and 2021Age groups overview of female CKD burdenThe age-specific DALYs rates for females due to CKD were highest for individuals aged 85 years or older in both 1990 and 2021 (Fig. 1, A and B). Between these years, the CKD burden for females significantly decreased among those under 15 years old and those 85 years or older. Among females aged 20 to 84 years, age-specific DALYs rates due to CKD saw a significant increase, with rates more than doubling for the 50 to 59 age group between 1990 and 2021.
Fig. 1
Age-specific rates of disability-adjusted life-years for females due to chronic kidney disease by age groups and sub-causes. Mexico, 1990 and 2021. YLLs: years of life lost (YLLs); YLDs: years lived with disability; T1D: type 1 diabetes; T2D: type 2 diabetes; AH: arterial hypertension; GN: glomerulonephritis; OTH: other/unknown causes. Source: own elaboration based on the GBD 2021
By sub-cause, the CKD burden in females under 15 years was primarily due to OTH. For those aged 15 to 59, GN was the leading sub-cause of CKD DALYs. In females aged 65 to 84, T2D was the main sub-cause of CKD, and AH was the leading cause for those over 85 years. The age-specific YLDs rates increased significantly among women aged 45–49 and those 85 years or older, while these rates decreased in females under 10. The age-specific YLLs rates followed the same pattern as the DALYs rates, with increases and decreases observed in the same age groups. Premature mortality (YLLs) had the highest percentage of the CKD burden in females between 50 and 74 years of age, while disability (YLDs) was highest in those aged 5–9 and 30 to 44 years of age (Fig. 1, C and D).
Subnational overview of female CKD burdenThe ASR-DALYs due to CKD for women in Mexican states in 1990 and 2021 are shown in Fig. 2 (A and B). In 2021, Tabasco, Veracruz, Yucatán, Tamaulipas, and Quintana Roo exhibited the highest ASR-YLDs when assessing premature deaths and disability separately. For 1990, Tabasco, Sonora, and Baja California Sur showed the highest ASR-YLDs due to CKD. Mexico City recorded the lowest ASR-YLDs both in 1990 and 2021. Between 1990 and 2021, the ASR-YLDs increased significantly only in Tabasco, while all other states experienced non-significant changes. In 1990, Guerrero, Puebla, Oaxaca, and Tlaxcala had the highest female ASR-YLLs. By 2021, Tabasco, Chiapas, Coahuila, Puebla, and Mexico State had the highest rates. In 1990 and 2021, Baja California Sur, Nayarit, and Sinaloa exhibited the lowest ASR-YLLs. On average, premature mortality accounts for approximately 90% of the total female ASR-DALYs due to CKD, while the rest is due to disability. In 2021, Tabasco, Veracruz, Yucatán, Tamaulipas, and Quintana Roo exhibited the highest ASR-YLDs when assessing premature deaths and disability separately. For 1990, Tabasco, Sonora, and Baja California Sur showed the highest ASR-YLDs due to CKD. Mexico City recorded the lowest ASR-YLDs both in 1990 and 2021. Between 1990 and 2021, the ASR-YLDs increased significantly only in Tabasco, while all other states experienced non-significant changes. In 1990, Guerrero, Puebla, Oaxaca, and Tlaxcala had the highest female ASR-YLLs. By 2021, Tabasco, Chiapas, Coahuila, Puebla, and Mexico State had the highest rates. In 1990 and 2021, Baja California Sur, Nayarit, and Sinaloa exhibited the lowest ASR-YLLs. On average, premature mortality accounts for approximately 90% of the total female ASR-DALYs due to CKD, while the rest is due to disability.
Fig. 2
Age-standardized rates of disability-adjusted life-years for females due to chronic kidney disease by states and sub-causes. Mexico, 1990 and 2021. YLLs: years of life lost (YLLs); YLDs: years lived with disability; NAT: National; AC: Aguascalientes; BC: Baja California; BCS: Baja California Sur; CM: Campeche; CS: Chiapas; CH: Chihuahua; CO: Coahuila; CL: Colima; CX: Mexico City; DG: Durango; GT: Guanajuato; GR: Guerrero; HG: Hidalgo; JC: Jalisco; MX: Mexico City; MI: Michoacán; MO: Morelos; NA: Nayarit; NL: Nuevo León; OA: Oaxaca; PU: Puebla; QT: Querétaro; QR: Quintana Roo; SL: San Luis Potosí; SI: Sinaloa; SO: Sonora; TB: Tabasco; TM: Tamaulipas; TL: Tlaxcala; VE: Veracruz; YU: Yucatán; ZA: Zacatecas. Source: own elaboration based on the GBD 2021
Over that period, a statistically significant increase in the female ASR-DALYs due to CKD for women in Mexican states in 1990 and 2021 was observed across 28 states. Chiapas, Tabasco, Veracruz and Tamaulipas experienced a surge of over 70% in the ASR-DALYs due CKD. On the other hand, the ASR-DALYs experienced a non-significant change in Mexico City, Querétaro, Colima, Jalisco, and Guerrero. In 2021, Tabasco and Chiapas (southern Mexico) had the highest female ASR-DALYs due to CKD. In contrast, Sonora, Baja California Sur, Nayarit, and Sinaloa (northwestern region) recorded the lowest ASR-DALYs (Fig. 2, A and B).
In 2021, across all states, sub-causes AH, GN, OTH, and T2D each accounted for a similar percentage (between 18.2% and 28.8%) of the total female ASR-DALYs (with GN and OTH representing more than 50%), while T1D contributed between 5.6% and 7.2% of the ASR-DALYs. These percentages were analogous in 1990 (Fig. 2, C and D).
Trend analysis of female CKD burdenNationally, the ASR-DALYs due to CKD for women significantly increased between 1990 and 2021 (AAPC of 1.0) (Table 2). In 29 states, a significant increase in the ASR-DALYs was observed, with AAPC ranging from 0.4 in Sonora to 2.2 in Tabasco. Guerrero was the only state that experienced a significant decrease (with an AAPC of -0.3). The national trend of the ASR-DALYs was segmented into four periods, whereas the subnational trends varied, ranging from four to a maximum of five. Nationally, there were several statistically significant periods showing changes in ASR-DALYs: an increase between 1996 and 1999 with an APC of 12.4%, a further rise between 1999 and 2009 with an APC of 2.5%, and a decrease from 2009 to 2021 with an APC of -2.4%. Most states experienced a significant rise in ASR-DALYs during the second period of the trend (around 1996–2000), with APCs ranging from 7.2% in Tamaulipas to 20.1% in Tabasco. Additionally, half of Mexico’s states saw another increase in the third segment of the trend, ending around 2009, with APCs ranging from 0.8% in Mexico City to 4.5% in Veracruz. Finally, in 2010, 24 states experienced a significant decrease in female ASR-DALYs due to CKD, with changes ranging from − 1.9% in Zacatecas to -5.6% in Quintana Roo.
Table 2 Joinpoint analysis of age-standardized rates of disability-adjusted life-years for females due to chronic kidney disease, by states. Mexico, 1990–2021Relationship between SDI and HAQI with female CKD burdenThe SDI and the HAQI increased in all states between 1990 and 2021 (Fig. 3). Nationally, we identified a significant positive correlation (0.64) between ASR-DALYs and the SDI. Additionally, 29 states showed a significant positive correlation between these measures. Sonora, Jalisco, and Guerrero were the states where the correlation was non-significant. These results suggest a linear association between sociodemographic development and the CKD burden among females in most regions of Mexico. Concerning the HAQI, we found a positive correlation (0.76) between this index and the female CKD burden. Almost all states, except for Guerrero, had a positive significant correlation between the HAQI and the ASR-DALYs. Moreover, the regression analysis showed that, at the national level and in most states, the ASR-DALYs due to CKD were significantly associated with the SDI and HAQI (Table 3).
Fig. 3
Correlation between age-standardized rates of disability-adjusted life-years for females due to CKD with Socio-Demographic Index and Healthcare Access and Quality Index by states. Mexico, 1990–2021. NAT: National; AC: Aguascalientes; BC: Baja California; BCS: Baja California Sur; CM: Campeche; CS: Chiapas; CH: Chihuahua; CO: Coahuila; CL: Colima; CX: Mexico City; DG: Durango; GT: Guanajuato; GR: Guerrero; HG: Hidalgo; JC: Jalisco; MX: Mexico City; MI: Michoacán; MO: Morelos; NA: Nayarit; NL: Nuevo León; OA: Oaxaca; PU: Puebla; QT: Querétaro; QR: Quintana Roo; SL: San Luis Potosí; SI: Sinaloa; SO: Sonora; TB: Tabasco; TM: Tamaulipas; TL: Tlaxcala; VE: Veracruz; YU: Yucatán; ZA: Zacatecas. Source: own elaboration based on the GBD 2021
Table 3 Linear regression between age-standardized rates of disability-adjusted life-years for females due to CKD with Socio-Demographic Index and Healthcare Access and Quality Index by states. Mexico, 1990–2021
留言 (0)