
記住我







This retrospective cohort study utilizes administrative claims data across three data sources in the United States using claims incurred between January 1, 2018 and December 31, 2020. The Center for Medicare and Medicaid Services (CMS) Medicare 100% Research Identifiable Files (RIF) contain all Medicare Parts A, B, and D paid claims incurred by 100% of Medicare fee-for-service (FFS) beneficiaries. The Milliman Contributor Health Source Data (CHSD) includes annual enrollment and paid medical and pharmacy claims for almost 25 million commercially insured individuals, 2.5 million Medicare Advantage beneficiaries, and over 5 million Managed Medicaid lives. The Merative Marketscan® Commercial dataset contains claims generated by 26 million commercially insured lives; this dataset supplemented Milliman’s CHSD for analysis of the commercial market with appropriate deduplication; data contributors who are included in the CHSD are prescreened and must confirm that they do not also contribute to Marketscan. Patients were assigned to one of four payer cohorts: Medicare FFS, Medicare Advantage, Medicaid, or commercial insurance.
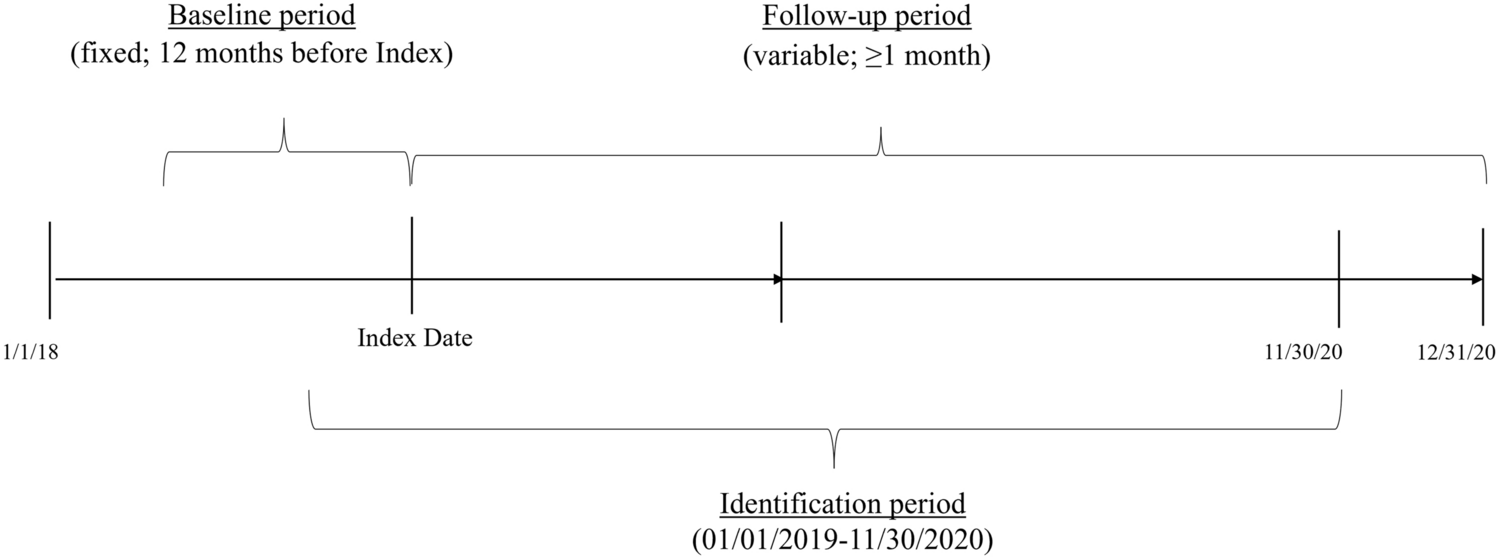
2.1 Study PopulationTo capture a prevalent patient population, patients were required to be diagnosed with and receiving treatment for PAH between January 1, 2019 and November 30, 2020 for inclusion in the study. A diagnosis of PAH was defined as (i) one or more inpatient or two or more outpatient claims ≥ 30 days apart with a PAH-related diagnosis code in any position (I27.0, I27.20, I27.21, I27.81, I27.89, I27.9) or (ii) a procedure for right heart catheterization (RHC) and an inpatient or outpatient claim with a PAH-related diagnosis code within 6 months before or after the procedure. The patient’s index date was determined as the earliest qualifying medical claim (by diagnosis or RHC procedure) or PAH-related therapy (ambrisentan, bosentan, macitentan, riociguat, tadalafil, sildenafil, iloprost, epoprostenol, selexipag, and treprostinil; all available formulations) during the identification period. Patients were not excluded from the study if previously diagnosed and treated. Treatments approved outside the analysis window (i.e., injectable selexipag, macitentan/tadalafil fixed-dose combination, and sotatercept) were not included in the study. Medicaid patients were required to have ≥ 10 months of enrollment in the 12 months leading up to index date for inclusion (i.e., 2 months of lapse in enrollment, both consecutive or independent, were allowed as Medicaid enrollees often incur brief lapses in coverage due to processes related to eligibility assessment [13]). All other patients were required to have continuous enrollment for ≥ 12 months prior to index date (i.e., baseline period) and at least 1 month following the index date for inclusion in the study (Fig. 1).
Fig. 1
Schematic of study design
Patients were excluded from the study if they were under 18 years of age or if they had any evidence of other PH subtypes (i.e., WHO Groups 2–5; diagnosis codes I27.22, I27.23, I27.24, I27.29 in any position, at any point during 2018–2020). Patients were followed from the index date until the end of enrollment, end of study period (i.e., 12/31/2020), or death (only known for Medicare patients due to data limitations), whichever occurred first.
2.2 Study MeasuresPatient demographics (age, sex), clinical characteristics (Quan-Charlson Comorbidity Index [QCI] [14], which assigns weights to select conditions and sums the results per patient, resulting in a score representing the risk of death from comorbid disease [15]), and prior PAH medication use by class were evaluated on the index date or during the baseline period, as appropriate. Comorbidities for the study population were identified via the CMS Hierarchical Condition Category (HCC) model (Medicare FFS) and the US Department of Health and Human Services (HHS) HCC models for index years 2019 and 2020, respectively [16, 17]. The ten most frequent comorbidities for PAH patients were aggregated across 2019–2020.
All-cause and PAH-related allowed (paid to the provider by both payer and patient; PAH-related where applicable), payer-paid, and patient OOP amounts (coinsurance, copay, and deductible) were summarized on a PPPM basis and are presented in terms of 2020 US dollars using the Consumer Price Index (CPI) [18], where applicable. Medical costs were summarized across the following service categories as average costs per patient per month: acute inpatient, pharmacy medication costs (PAH vs non-PAH), non-pharmacy medication costs (covered under the medical benefit; PAH vs non-PAH), and all other all-cause medical costs ‘other’. In the Medicare FFS and Medicare Advantage cohorts, pharmacy costs were summarized using Part B and Part D claims. While payer-paid amounts on Part B claims reflect the amounts paid by the payer, due to multiple sources of funding in Part D, payer-paid amounts on Part D claims reflect all amounts not paid by the patient. Rates of acute inpatient admission were calculated on a per-1000-patients basis. PAH-related admissions were identified as those with a PAH-related primary diagnosis code (I27.0, I27.20, I27.21, I27.81, I27.89, I27.9). All-cause and PAH-related utilization and average costs per admission for the first observed and subsequent acute inpatient admissions were assessed.
All study measures were assessed and are presented separately by payer cohort (i.e., Medicare FFS, Medicare Advantage, Medicaid, and commercial) and reflect the entire experience of the study population from index date through end of follow-up or censor. Parenteral prostacyclin therapy within 30 days of the index date was identified as a marker of advanced disease, and results were stratified accordingly for the commercial and Medicare FFS cohorts. National-level burden estimation was carried out by (i) determining national payer-specific patient counts by applying prevalence rates of PAH obtained from this study to national enrollee counts and (ii) multiplying the annualized medical and pharmacy PPPMs obtained from this study to the 2021 national adult enrollment estimates (electronic supplementary material [ESM], Table 1).
2.3 Statistical AnalysisOutcome measures were summarized beginning with the index date through the earliest of (i) the end of continuous enrollment, (ii) date of death (Medicare FFS only), or (iii) end of the study (i.e., December 31, 2020). Continuous measures were presented as descriptive statistics and categorical measures were presented as proportions/percentages. Mean and median values were calculated for PPPM payer and OOP costs. Mean, median, and standard deviation (SD) values were calculated for all-cause and PAH-related inpatient admissions per 1000 patients and for per-inpatient admission costs. No hypothesis testing was conducted. All analyses were carried out using SAS software, Version 9.4 (Copyright © 2013 SAS Institute Inc. SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc., Cary, NC, USA).
留言 (0)