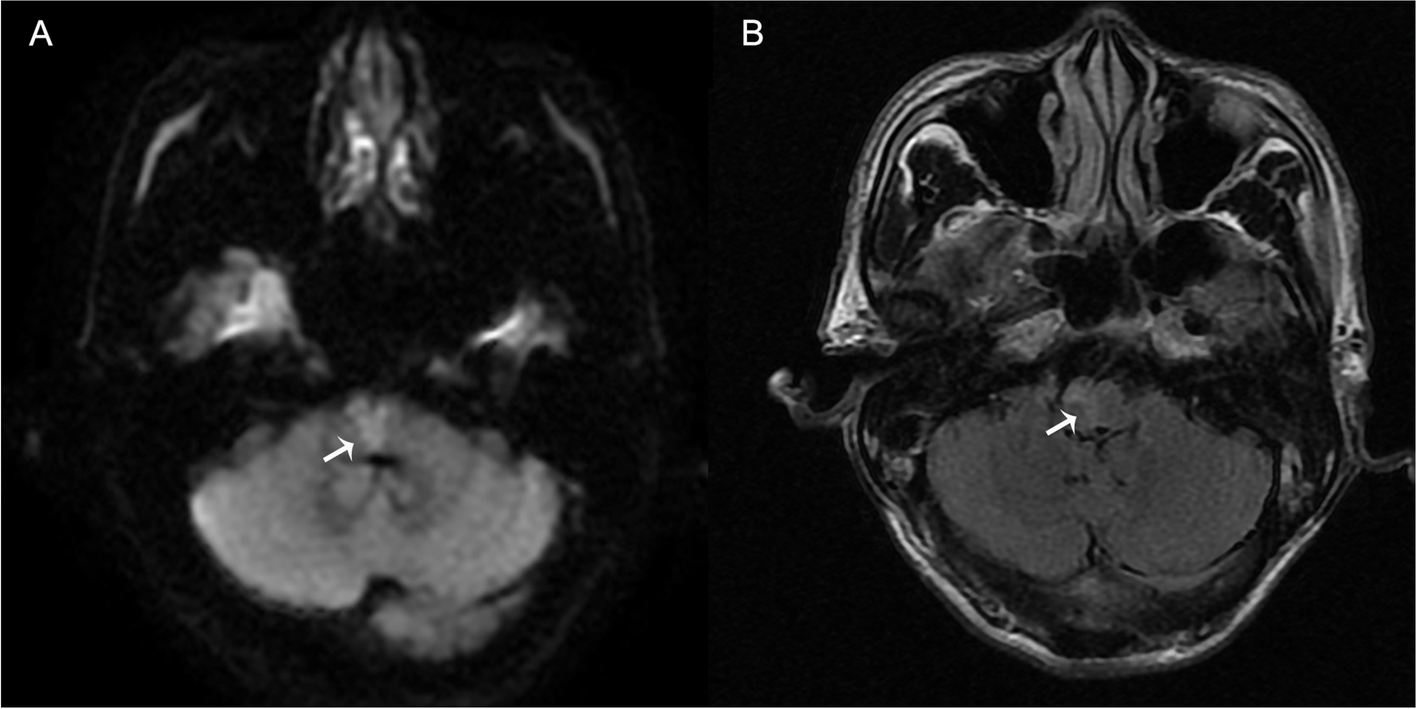
ET, a rare etiology of IS, is thought to arise via two distinct pathways [11]. First, when ET coincides with cerebrovascular disease risk factors, such as AS, these factors can exacerbate vascular stenosis and occlusion, thereby increasing the risk of IS. Secondly, ET can trigger increased platelet activation and aggregation, thus promoting thrombotic events. ET-induced thrombosis often manifests as multiple infarcts that concurrently affect various vascular regions. Our patient presented with a combination of AS risk factors including hypertension, smoking, and hyperhomocysteinemia. Despite this, the patient’s platelet count on admission exceeded 1500 × 109/L and DWI sequencing revealed multiple cerebral infarctions. Hence, we hypothesized that IS in this patient was primarily attributable to ET-induced thrombosis. What was even more interesting was that the patient underwent splenectomy which was due to a splenic infarction combined with a splenic abscess, and the reason for the splenic infarction was believed to be caused by ET which was confirmed in subsequent treatment. Therefore, the thrombocytosis in this patient was considered to be co-caused by ET and splenectomy after splenic infarction due to ET, which further resulted in cerebral infarction. Moreover, the literature has indicated that IS resulting from ET predominantly manifests as watershed and lacunar infarctions [7], predominantly affecting the anterior circulation [12], whereas occurrences in the infratentorial area are exceedingly rare [6, 7]. Our patient had a BMMI with an incidence rate of approximately 0.1% [8, 13].
BMMI is often referred to as “heart appearance” or “Y appearance” infarction. Currently, it is understood that “Y appearance” infarction is commonly associated with lesions in the perforating arteries, and typically results from three primary vascular pathological mechanisms: Thrombus originating from the distal unilateral VA and traversing to the contralateral side through the junction of the vertebrobasilar artery, and blood supply from the narrow or occluded paramedian branches originating from the unilateral VA or bilateral anterior spinal arteries (ASA) originating from the unilateral VA to the bilateral medial medulla due to anatomical variations [8, 14]. Normally, the blood supply to the superior one-third of the anterior-medial territory of medulla oblongata comes from the VA and the inferior two-thirds comes from the ASA [15]. The infarction site in this patient was located in the rostral medulla, so occlusion of the ASA was not considered the cause. The patient’s MRA revealed that the left VA was small, indicating left vertebral artery hypoplasia (VAH). Although the blood flow in the VAH is significantly reduced, there is no sign of ischemia due to the compensatory effect of the contralateral VA [16]. Moreover, research suggests that VAH may be associated with variations in the posterior cerebral arterial structure [17]. Though MRA cannot demonstrate the presence of posterior circulation perforating arteries, we believe it is more likely that this patient’s blood supply to the bilateral medial medulla was from the narrow or occluded paramedian branches originating from the unilateral VA due to anatomical variations. Furthermore, based on the anatomical arrangement of the medulla oblongata, the medial aspect consists of the pyramidal tract, medial thalamus, medial longitudinal fasciculus, hypoglossal nucleus, and vestibular nucleus in a ventral-to-dorsal sequence [9]. Based on the patient’s signs and symptoms, such as decreased muscle strength, increased muscle tone, hyperreflexia of the tendons, and positive ankle clonus, these findings were presumed to be associated with pyramidal tract involvement. This decrease in sensation is attributed to the involvement of the medial thalamus, whereas dizziness and nystagmus are closely associated with the medial longitudinal fasciculus and vestibular nucleus. The patient’s symptoms, including dysphagia, coughing upon drinking water, and articulation disorders, suggest that ischemia may extend to the lateral aspect of the medulla oblongata, thereby affecting the nucleus ambiguus and cortical medullary tract. In summary, based on the patient’s symptoms, signs, and imaging findings, the diagnosis of “Y appearance” infarction was clear.
According to the Chinese Experts Consensus on Clinical Application of Tirofiban in Atherosclerotic Cerebrovascular Diseases, we administered intravenous antiplatelet therapy with tirofiban. Tirofiban, functioning as a glycoprotein IIb/IIIa receptor antagonist, inhibits platelet aggregation by blocking interactions between platelets and fibrinogen [18]. Because of its rapid onset of action during administration and prompt recovery upon cessation, tirofiban typically does not substantially increase the risk of bleeding events, but can effectively prevent thrombosis [19]. This treatment is currently recommended for patients with progressive stroke caused by small artery occlusion, and the duration of administration is at least 24 h. Our patient initially exhibited a decrease in muscle strength after switching to aspirin following 72 h of tirofiban use. Additionally, the patient’s platelet count consistently exceeded 1300 × 109/L, which increased the risk of bleeding and thrombus formation in the blood vessels of various organs. Therefore, considering various factors, we continued to use tirofiban for 14 days until the patient’s condition stabilized. This approach aims to prevent further deterioration and mitigate the continued activation and aggregation of platelets. In general, the prognosis of patients with BMMI is poor and characterized by limited recovery potential and a high mortality rate [20]. Nevertheless, after long-term tirofiban and other symptomatic supportive treatments, the patient showed remarkable improvement. At the latest follow-up, the patient showed only limb numbness. This is a particular case of “Y appearance” infarction treated with high-dose tirofiban, resulting in a favorable prognosis.





留言 (0)