
記住我




A 36-year-old woman was admitted to the hospital following a series of recurring episodes characterized by exertional chest tightness and pain that had persisted for more than a year. She had a long-standing history of hypercholesterolemia dating back to the age of 7, at which time she had already developed multiple nodular xanthomas, a clear indication of her underlying lipid disorder. Notably, despite being suspected but not diagnosed with HoFH at the age of 7, she did not initiate statin therapy until the age of 32. During this 32-year period, the patient did not receive any lipid-lowering treatment, suggesting that she may have had a relatively mild phenotype of HoFH.
At the age of 32, in an attempt to manage her persistently elevated LDL-C levels, she initiated the maximum tolerated statin therapy, specifically rosuvastatin at a daily dosage of 20 mg. however, achieving effective control remained an elusive goal. Despite the subsequent addition of ezetimibe and evolocumab to her treatment regimen, her LDL-C levels fluctuated between 12–14 mmol/l, highlighting a refractory response to conventional therapies. Genetic testing revealed a homozygous LDLR mutation at c.1104C > A (p.C368X), providing a molecular explanation. Remarkably, throughout this, she remained asymptomatic.
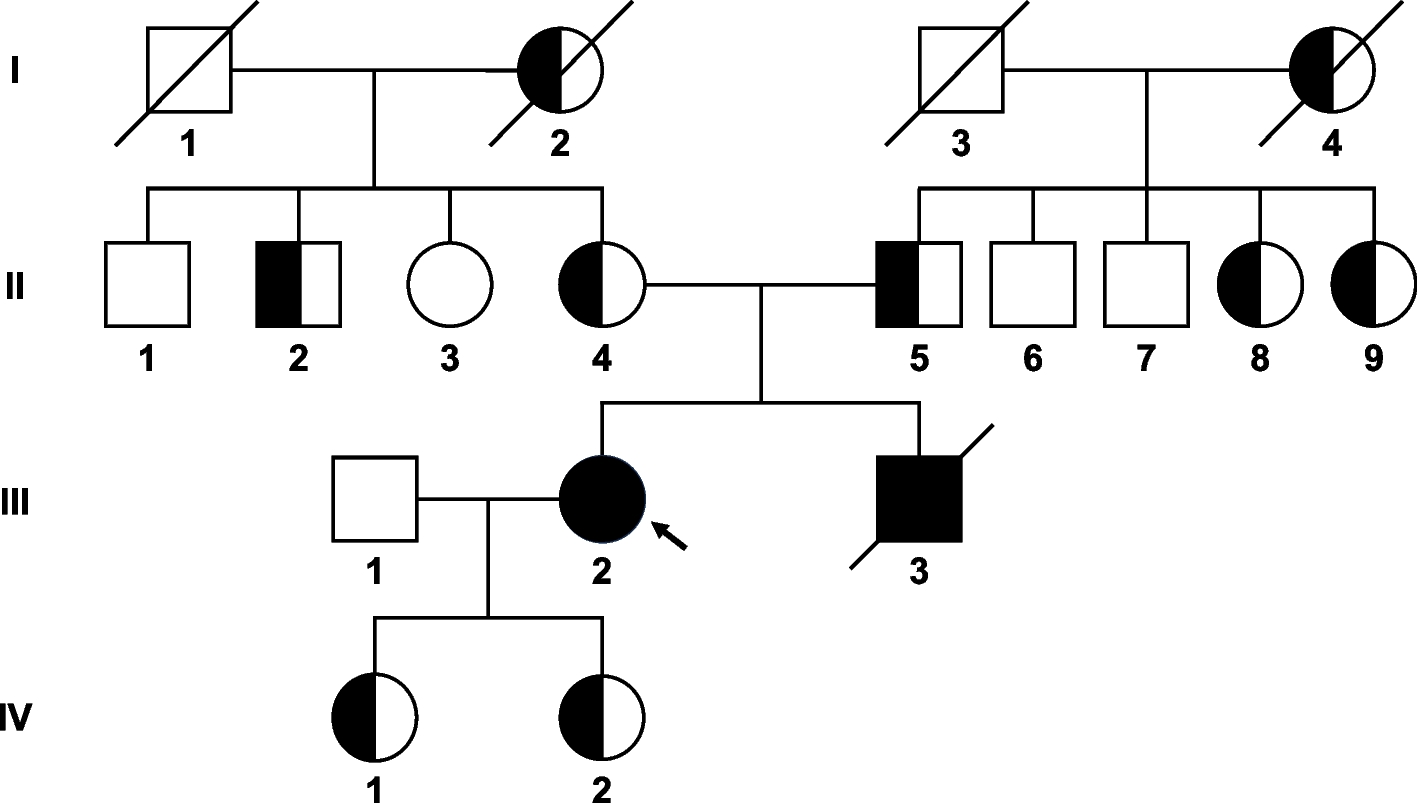
At the age of 35, the patient started to endure recurrent episodes marked by chest tightness and pain, which were triggered by physical exertion or emotional excitement. Each episode persisted for 2–3 min and was alleviated by rest. These distressing occurrences necessitated hospitalization for comprehensive treatment in February 2022. Her family history revealed a consanguineous marriage in her parental lineage, a potential risk factor for the development of her condition. she had a brother who succumbed to sudden death at the age of 25 following an episode of heavy alcohol consumption, also presenting with xanthomas and had markedly elevated LDL-C levels of approximately 20 mmol/L, but his condition remained undiagnosed and untreated. Furthermore, genetic testing confirmed that both her parents, daughters, two aunts, as well as one uncle, were carriers of the LDLR gene mutation at the c.1104C > A (p.C368X) site, indicating they have HeFH (Fig. 1A).
Fig. 1
Pedigree of the present familial hypercholesterolemia family. The proband is indicated by an arrow. Squares indicate males; circles, females; slashes, deceased individuals; shaded (black) symbols, individuals with homozygous familial hypercholesterolemia; half-shaded (black) symbols, individuals with heterozygous familial hypercholesterolemia. I-2 and I-4 are full sisters
Physical examination revealed multiple large nodular xanthomas on her limbs, waist, and buttocks, further corroborating her clinical presentation (Fig. 1B). Auscultation detected a diastolic murmur at the aortic valve area and a grade 2 soft systolic murmur at the left sternal border between the 3rd and 4th ribs, indicative of potential valvular involvement. Laboratory findings showed markedly elevated LDL-C levels of 13.2 mmol/l and total cholesterol (TC) levels of 15.7 mmol/l.
Following treatment initiation, the patient underwent once every 1–2 months LA via peripheral venous access (Fig. 2A). Double filtration plasmapheresis (DFPP) was performed using an OP-08W plasma separator with an EC-50W filter, blood flow 100–130 mL/min, sessions lasting 3–4 h. Over two years, 12 DFPP sessions were conducted, totaling 45 h. The patients tolerated the DFPP treatment well, with no serious adverse reactions observed. Occasional mild dizziness and fatigue were reported during the treatment process, but these did not require interruption of the treatment. The cost of each DFPP treatment session was approximately 7,000 RMB. Pre-DFPP, LDL-C and TC were 13.82 ± 3.28 and 15.45 ± 0.78 mmol/L, respectively. Post-DFPP, LDL-C and TC significantly decreased to 2.43 ± 0.33 and 3.59 ± 0.41 mmol/L with reductions of 81.76 ± 4.11% and 76.76 ± 2.75%. Lipoprotein (a) (Lp(a)) and triglycerides (TG) also significantly decreased by 89.10 ± 1.39% and 42.29 ± 15.68%. Pre-DFPP, albumin and globulin were 41.30 ± 1.92 and 29.36 ± 1.99 g/L. Post-DFPP, they decreased to 34.16 ± 2.67 and 18.31 ± 2.30 g/L (17.14 ± 7.11% and 37.54 ± 7.62% reductions),globulin levels showed a mild decrease (Fig. 2B).
Fig. 2
The clinical follow-up of the patient. A The direct puncture technique, procedure, and disposal of waste plasma during DFPP therapy. B Changes in low-density lipoprotein cholesterol(LDL-C, mmol/l), total cholesterol(TC, mmol/l), albumin(ALB, g/l), and globulin(GLB, g/l) levels pre and post DFPP therapy. C Echocardiography manifestations: The times of four examinations (2021–12-14 outpatient, 2022–02-09 first DFPP, and two follow-ups on 2022–06-21/2023–06-29) showed irregular thickening and calcification protruding into the lumen at the sinotubular junction of the aortic root, causing localized stenosis. Transaortic maximum velocity (Vmax) and mean paravalvular gradient (PGmean) were recorded for assessment, as transaortic Vmax was 2.9 m/s, PGmean was 18 mmHg (2021–12-14); transaortic Vmax was 3.0 m/s, PGmean was 20 mmHg (2022–02-09); transaortic Vmax was 3.4 m/s, PGmean was 22 mmHg(2022–06-21); transaortic Vmax was 3.1 m/s, PGmean was 20 mmHg(2023–06-29), respectively. D Carotid artery ultrasound manifestations: The times of the two examinations (the first DFPP on 2022–02-14, and a follow-up on 2023–06-30). The results showed moderate to severe stenosis at the origin of the right internal carotid artery (RICA). The peak systolic velocity (PSV) was recorded at the origin and distal end of the RICA, as well as the intima-media thickness (IMT) of the right common carotid artery (RCCA), and the PSV and Velocity Ratio (Vr) changes before the right common carotid artery stenosis (RCAS). The values were: RICA proximal was PSV 268 cm/s, RICA distal PSV was 109 cm/s, RCCA IMT was 1.2 mm, before RCAS PSV was 110 cm/s, 2 < Vr < 4 (2022–02-14) and RICA proximal PSV was 222.5 cm/s, RICA distal PSV was 103 cm/s, RCCA IMT was 1.4 mm, before RCAS PSV was 85 cm/s, 2 < Vr < 4 (2023–06-30)
Simultaneously, Echocardiography at the same period: Calcification of the aortic sinus-ascending aorta junction with associated stenosis, internal diameter narrowed to about 14 mm. The aortic sinus was relatively narrow at about 25 mm. Accelerated antegrade flow at the aortic sinus-ascending aorta junction with the transaortic maximum velocity (Vmax, 3.0 m/s) and the mean transvalvular pressure gradient (PGmean, 20 mmHg). Bicuspid aortic valve thickened and calcified with associated regurgitation, annulus diameter of about 21 mm (Fig. 2C). Bilateral carotid artery ultrasound showed: Bilateral carotid artery intima-media thickening, with a thickness of about 1.2 mm on the right side and 1.2 mm on the left side. The intima-media thickness at the origin of the right subclavian artery was about 1.3 mm. The right internal carotid artery showed stenosis at the origin, with a weak echogenic plaque of 3 mm thickness and increased blood flow velocity, with a peak systolic velocity (PSV) of 268 cm/s. No stenosis was observed in the left carotid artery (Fig. 2D). During the hospitalization, coronary angiography revealed severe calcific ostial stenosis of approximately 95% in the left main coronary artery (LMCA). There was an 80% stenosis in the proximal left anterior descending artery (LAD) and a 70% stenosis in the mid-LAD segment. The right coronary artery (RCA) had a 70% stenosis in the mid-segment and a total occlusion in the distal segment. Consequently, two drug-eluting stents were sequentially implanted from the LMCA to the LAD to restore blood flow. Additionally, three drug-eluting stents were placed in the RCA to revascularize the affected segments and restore coronary perfusion.
During the follow-up period after initiating DFPP treatment, the patient's aortic stenosis and stenosis of the carotid arteries, right subclavian artery, and right internal carotid artery did not worsen significantly. Coronary angiography confirmed the patency of the previously implanted stents, with no evidence of in-stent restenosis.
Furthermore, we summarized the research studies on using LA to treat familial hypercholesterolemia (FH), with a particular emphasis on the pros and cons of LA (Table 1).
Table 1 Summary of the research studies on using Lipoprotein Apheresis (LA) to treat Familial Hypercholesterolemia (FH)
留言 (0)