General Characteristics
CA included n = 185 patients and CB included n = 58 patients. A total of n = 135 patients (72.97%) in CA and n = 40 patients (68.97%) in CB had no residual tumor at the end of debulking surgery. Severe complications (G3–G5) were seen in n = 56 patients (30.2%) in CA and in n = 10 patients (17.2%) in CB. In total, there were n = 117 patients with anastomoses and n = 149 anastomoses (n = 86 patients with n = 1 anastomosis, n = 30 patients with n = 2 anastomoses, and n = 1 patient with n = 3 anastomoses). Anastomotic leakage was seen in n = 16 patients out of n = 91 patients (17.6%) in CA and in n = 3 out of n = 26 patients (11.5%) in CB (p = 0.188). There were n = 3 ALs in a total of n = 38 anastomoses (7.9%) in CB and n = 16 ALs in n = 111 anastomoses in CA (14.4%). Only n = 1 AL was at a PFE of less than 3000 ml. There was no significant difference between both cohorts regarding surgical complexity, tumor load (by PCI and FIGO stage), ASA score, or the number of intestinal resections and anastomoses. CB patients were significantly older, were less frequently treated with neoadjuvant chemotherapy and exhibited a shorter duration of surgery, as depicted in Table 1. Furthermore, CB patients required significantly less postoperative intensive medical care and less postoperative ventilation. Length of hospital stay was significantly reduced in CB patients (Table 2). CB patients showed no increase in severe (G3–G5) complications (p = 0.063) or anastomotic leakage (p = 0.556). Ultrasevere complications (G4–G5) were exclusively seen in CA patients (p = 0.0255). CA patients received a median of 0 whole blood transfusions (range: 0–14) and a median of 0 fresh frozen plasmas (FFP) (range: 0–18). CB patients received a median of 0 whole blood transfusions (range 0–3) and 0 FFPs (range: 0–8).
Table 1 Patient demographics and surgical details of cohorts A and BTable 2 Postoperative outcome data, intraoperative fluid differences, and noradrenalin amountPFE
Intraoperatively, CB patients received significantly more noradrenalin and had a significantly lower median PFE as depicted in Table 2. Both cohorts showed a significant increase in the PFE in case of a PCI > 10, but again the increase was significantly lower in CB patients. Comparing FIGO stages only, there was no significant increase of the PFE in CB patients. In CA patients there was a significant increase in the case of FIGO stages greater than IIIB.
In general, severe complications (G3–G5) and anastomotic leakage increased with increasing fluid load as depicted in Table 3. Further reasons for significant more severe complications (G3–G5) were a FIGO stage greater than IIIB (p = 0.004), a surgical complexity score of > 2 (p = 0.027), the presence of anastomoses (p < 0.001), and a pre- and postoperative hemoglobin difference of equal to or more than 3 g/dl, as shown in Table 4. AL rates were not affected by increasing hemoglobin differences (≤ 3g/dl; p = 1.000, ≤ 4 g/dl; p = 1.00, ≤ 5 g/dl; p = 0.064). Shorter times to first defecation were seen in CB patients (p = 0.001), in case of a PFE less than 5000 ml (p = 0.001) and in case of a preoperative bowel preparation with antibiotics (p = 0.001). In total there were 37 loop ileostomies (31.6%) performed, 29 in CA and 8 in CB.
Table 3 Association of fluid balance with severe complications (G3–G5) and anastomotic leakageTable 4 Association of the postoperative hemoglobin difference with severe complicationsDiscussion
These two unselected real-world cohorts demonstrate that an intraoperative fluid restriction according to a PPVGHM, achieved by an increased use of noradrenalin, is possible without increasing severe complications in patients with ovarian cancer. In fact, ultrasevere complications (G4/G5) were exclusively seen in CA with liberal fluid management. In general, intraoperative fluid reduction led to earlier postoperative defecation, shorter length of hospital stays, and less intensive care need. No acute kidney injury was observed in the whole PPVGHM cohort.
Fluid overload and fluid restriction are established risk factors regarding postoperative complications in abdominal surgery.17,18 Current recommendations of the ERAS society restrict fluids to a maximum postoperative weight gain of 2.5 kg in colorectal surgery.11 There is no such recommendation in patients with ovarian cancer yet.19 Consistent with the above-mentioned recommendations, we observed a significant increase of complications beginning at a PFE of 3000 ml.11 A recent analysis from the Karolinska Institute from Sweden also found increasing complications at a net fluid balance at 3000 ml, 48 h after surgery.14 The net fluid balance was defined as the sum of all administered fluids including blood products minus all fluid losses including blood, urine, and ascites.14 In our analysis, the positive fluid excess was defined as the sum out of all administered crystalloids and colloids minus the urine output. We did not consider ascites or blood loss to keep the parameter as simple as possible. Ascites was not considered, as this volume is neither intracellular nor intravascular, and therefore excluded from the organ perfusion anyway. Blood loss was not considered as this is, besides a spectrophotometric measurement a rather roughly estimated parameter and therefore of limited reliability especially in patients with advanced-stage ovarian cancer.20 Furthermore, advanced-stage ovarian cancer patients show an intraoperative capillary leak and intravascular hypoalbuminemia, consecutively leading to intra-abdominal extravasation and enormous intercompartmental fluid losses.13 To maintain hemodynamic stability in these cases, fresh frozen plasmas are recommended to be transfused without resemblance to blood loss.21 Consecutive blood replacements are based on intraoperative hemoglobin levels and the amount of fresh frozen plasmas transfused, rather than on the estimation of the blood loss during surgery and the circulatory situation itself. The ESGO guideline recommends a liberal policy regarding the transfusion of blood products.12
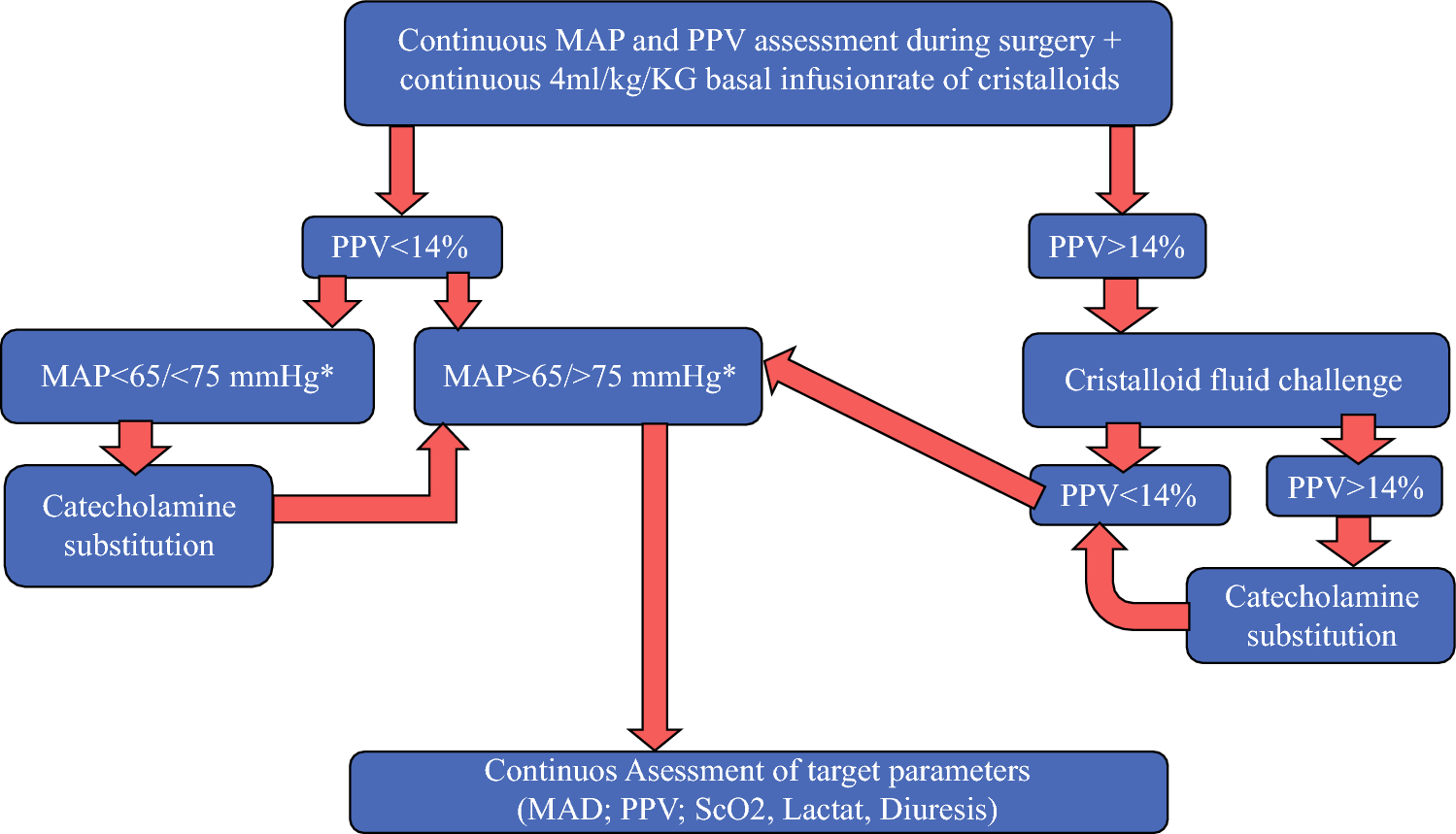
Recently, two different pathways have been introduced to optimize the intraoperative fluid management in abdominal surgery and ovarian cancer surgery, i.e., goal-directed hemodynamic management and goal-directed fluid management. The goal-directed hemodynamic management is based on pulse pressure variations and stroke volume variations as main indicators of the fluid responsiveness of patients during surgery. In patients with ovarian cancer this led to shorter length of hospitalization, shorter times to first postoperative defecation and lower blood lactate levels, postoperatively.15 The goal-directed fluid therapy is based on the near maximal stroke volume as the main indicator for fluid replacement.22 In abdominal surgery, for various reasons, no positive effect on the postoperative outcome has been seen so far.22 The ESGO guideline of the perioperative management of patients with ovarian cancer defines no cutoff for a maximum of intraoperative fluids so far.12 The PPVGHM in CB patients led to a median PFE of no more than 3150 ml even in the high tumor load group with a PCI of ≥ 10. The PPV has been identified as a precise marker for fluid responsiveness, easy to monitor and more reliable than systolic pressure variations or the pulse contour stroke volume variation.23 The PPV displays the position on the Frank–Starling curve, where the patient’s heart is operating. If it is operating on the plateau, preload and contractility are at their optimum and the PPV is low. In case of operating on the steep part of the curve, where the preload is decreasing, the PPV increases. Nevertheless there are also several limitations for the use of the PPV regarding volume expansion or volume depletion as cardiac arrythmia, active breathing, and very low tidal volumes.23
Regarding ALs, CA showed an AL rate of 17.6% accompanied by a significantly higher median PFE of 5200 ml compared with CB with an AL rate of 11.6% with a median PFE of 2598 ml. In the whole population, significantly more anastomotic leakages were seen at a PFE ≥ 4000 ml. In fact, only one AL was seen at a PFE of less than 3000 ml. The AL rate in CB dropped, despite a more unfavorable population with a median age of 67 and a mean age of 64.5 years and a higher rate of additional small bowel resections of 46.2% by reducing fluids. This compares favorably with Lago et al., who showed that age and additional small bowel resections were significant risk factors for AL in the multivariate analysis.24 The AL range at those eight centers of Lago et al. was 1.7–12.5% in a more favorable cohort with a mean age of only 58.7 years and a rate of additional small bowel resections of only 8.9%. CA was also less favorable, with a mean age of 60.5 years and a rate of additional small bowel resections of 20.9%, but also received significantly more fluids. Analyzing the surgical expertise in numbers, our data are comparable with the data of Lago et al.24 The average number of patients per center per year with anastomosis was 11.6, considering that 695 patients from 8 centers within 7.5 years were analyzed. In detail, the performance of an anastomosis ranged from 3.5 to 18.7 patients per center per year.24 The average number of patients with an anastomosis was 14.6 out of 30.4 patients undergoing cytoreduction per year in our center, in a less favorable cohort.
Regarding anastomoses, the fluid overload leads to at least three consequences. First, the positive fluid excess leads to more intraabdominal pressure and less tissue circulation due to a splanchnic edema..10,25,26 Second, the structural and functional stability of anastomoses is altered with increasing fluid quantity, and the needed pressure to accomplish anastomotic bursting decreases.27 Therefore, it seems of imminent importance to further explore the entire postoperative fluid management in addition to that, as the first bursting pressure for an anastomosis will be on day 2 or 3 and ALs are generally recognized on days 5 to 8.28 The third consequence of a fluid overload by crystalloids is hemodilution, altering anastomotic healing due to a decreased oxygen supply if not balanced postoperatively to hemoglobin levels above 10 g/dl.29 In our cohorts we saw an association of pre- and postoperative hemoglobin differences of equal or greater than − 3 g/dl and an increase in severe postoperative complications. We did not observe more ALs, which may be related to the small sample size of ALs and due to a very liberal transfusion of blood within the postoperative course. While preoperative anemia is a known risk factor for postoperative adverse events, postoperative anemia has just recently been identified as risk factor for postoperative complications.17 Regarding intestinal anastomoses, it is associated with altered anastomotic healing in the small and the large bowel.30 Whether generous whole blood transfusions can modify this observation has not yet been answered due to scarce data regarding this question.
In accordance with previous studies we saw more complications in cases where there was creation of anastomoses, as surgical complexity increased, and as FIGO stage increased.8,31
Our study is limited by its retrospective design and its sample size, both potentially being confounding factors. Significant differences between cohorts were the application of neoadjuvant chemotherapy, the age of the patients, and the operating times. The difference in the use of neoadjuvant chemotherapy is due to the prior policy of the clinic to administer neoadjuvant chemotherapy in case of ascites of more than 500 ml until 8/2019. The age difference is most probably due to the retrospective real-world cohorts. No patient scheduled for cytoreduction was excluded. The shorter operating times in cohort B are probably due to the same reason. But of course, we cannot exclude any bias here.
Furthermore, we evaluated only the intraoperative fluid management, excluding the postoperative fluid management until patients were fully recovered. Due to the retrospective design, we were not able to provide a detailed description of the factors leading to fluid management before implementing the new standard of care in 2021.
A strength of our study is the homogeneous patient population and the simple parameters used for optimization of the fluid management, which makes our PPVGHM easy to implement into the routine intraoperative management of ovarian cancer patients. Further prospective studies are urgently needed to optimize the intra- and postoperative fluid management in patients with ovarian cancer. This is emphasized by the fact that fluid management has been recognized as modifiable risk factor, while comorbidities of patients and the goal of complete cytoreductive surgery are set parameters in the fight against postoperative complications and for survival in ovarian cancer patients.


留言 (0)