All bariatric patients were treated according to international guidelines [4]. Patients with large hiatal hernias (Type IV; > 5 cm length) and BMI > 35 kg/m2 were offered simultaneous hiatal hernia repair during RYGB. Esophago-gastro-duodenoscopy was performed prior to bariatric surgery in all patients.
Radiological diagnostics
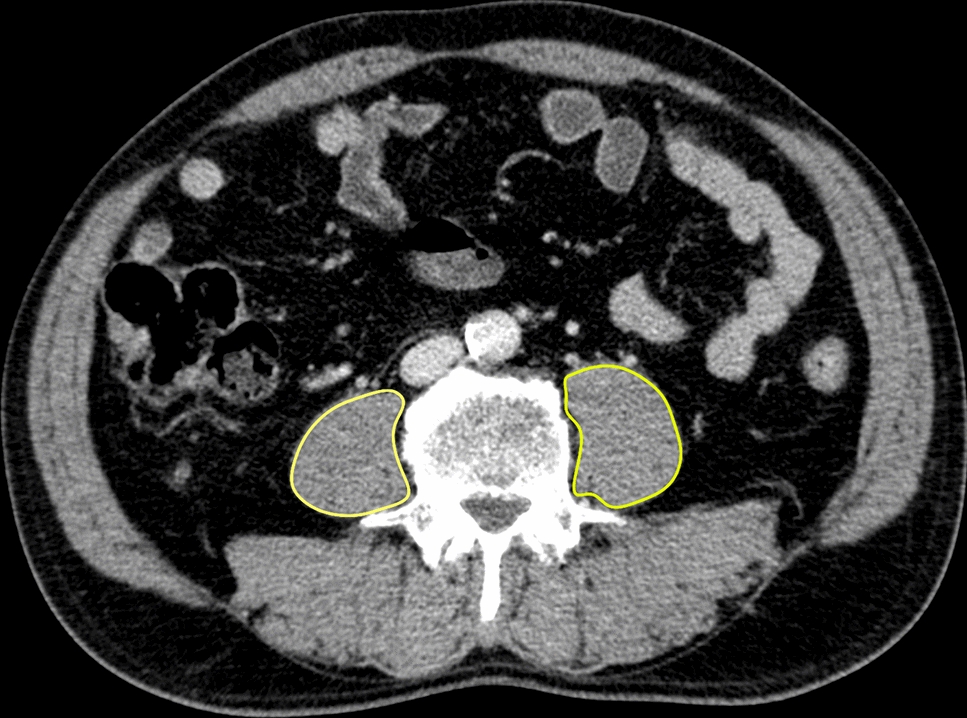
Radiological assessment was performed by an experienced radiologist using syngo.via™ post-processing software with the auto-contouring algorithm 3D Lesion Segmentation (Siemens Healthcare GmbH, Erlangen, Germany).
Surgical technique
All surgeries were performed laparoscopically in beach chair position by an experienced upper gastrointestinal and certified bariatric surgeon. Four trocars and a liver retractor (Mediflex®) were used.
Roux-en-Y gastric bypass was created in an antecolic and antegastric fashion, with the greater omentum being divided. The length of the Roux and biliopancreatic limb was 120 cm and 80 cm, respectively. The entero-entero-anastomosis (EEA) was created side to side using a linear stapler.
In the case of a large hiatal hernia, a full dissection of the hernia sac was performed until tension-free intra-abdominal positioning of the gastroesophageal junction was accomplished. If a pleural lesion occurred, the capnoperitoneum pressure was reduced, while the positive end-expiratory pressure (PEEP) was increased accordingly to prevent the necessity of a chest tube. During full dissection of the hernia sac, the short gastric vessels were preserved to maintain sufficient blood supply to the fundus. A posterior hiatoplasty was performed, while a 36 Charriere bougie was used for calibration.
A small pouch (30 mL) was created, and a side-to-side gastro-jejunostomy (GJ) using a linear cutting stapler was performed. The defect was closed with running resorbable 3/0 sutures. The mesenteric gaps were closed with running non-resorbable sutures.
Data assembly and statistical analyses
From January 2012 until December 2022, 573 consecutive RYGB surgeries were performed. Of those, 12 patients received simultaneous treatment for a large hiatal hernia (Hill Type IV; > 5 cm length).
The primary end point was overall complication measured by the Clavien–Dindo-comprehensive complication index [5]. Secondary end points were duration of surgery, reoperation rate, length of stay, and recurrence of hiatal hernia.
Statistical analyses were performed using IBM SPSS Statistics 29 (International Business Machines Corporation, Armonk, NY). Descriptive data were reported as means with standard deviations, unless otherwise stated. Comparisons between the analyzed cohorts were performed using Chi-square, Fisher’s exact, and Mann–Whitney U tests or one-way analysis of variance, in accordance with data scale and distribution. The level of statistical significance was 0.05.




留言 (0)