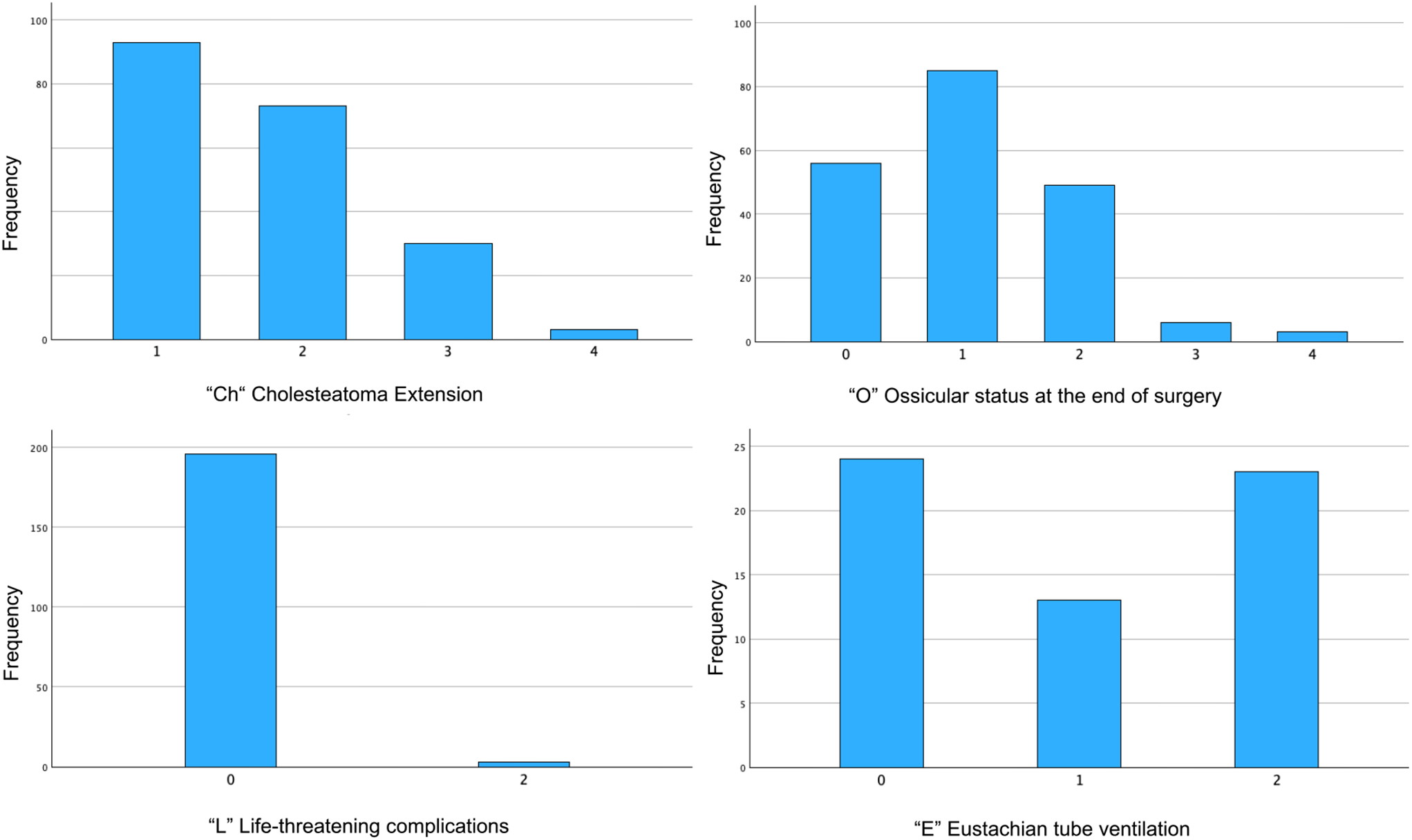
Our study population of 199 patients exhibited a notable distribution of cholesteatoma stages, with stage 1 being the most prevalent, followed by stage 2, and no cases classified as stage 3. Moreover, we identified a significant correlation between the stages of cholesteatoma extension (Ch) and the duration of surgery. As the stage of extension increased, so did the duration of the surgery. Furthermore, our analysis revealed significant correlations between the ossicular chain status at the end of surgery (O), life-threatening complications (L), mastoid pneumatization (E), and the duration of surgery. These findings underscore the comprehensive nature of the classification, which considers various factors influencing complexity of procedure and emphasizes the ability of the ChOLE Classification System in assessing the extent of cholesteatoma, predicting surgical complexity, and thus guiding surgical decision-making.
The distribution of subgroups within the ChOLE Classification in our study exhibits both resemblances and disparities in comparison to previous research conducted [4, 9]. In our study, stage 1 cholesteatoma was the most prevalent. However, in the studies conducted by Hajare et al. and Weiss et al., stage 2 cases were more prevalent [4, 9]. Concerning the specific ChOLE classifications, our study revealed similar proportions of Ch1a and Ch1b, and Ch2a and Ch2b cases compared to Hajare et al., suggesting comparable patterns of middle ear involvement extending to the sinus tympani across both studies. Similarly to our findings, Hajare et al. also reported Ch4 to be the least frequent subgroup among the studied population. However, Ch3 was the most frequent extension, whereas our study showed Ch1 to be the most frequent one. Weiss et al. reported a different distribution of the Ch subgroup, with stages 1 and 2 being the most frequent ones, followed by stage 4 and then stage 3, indicating potential differences in surgical techniques or patient populations [9]. In terms of ossicular chain status (O), our study found a high prevalence of malleus and stapes present with eroded incus (O1) and a low prevalence of fixed stapes (O4), consistent with findings from Weiss et al. and Hajare et al. [4, 9].
Life-threatening complications (L) were infrequent in our study, with no cases of intracranial complications (L4) described, whereas Hajare et al. described one case of a brain abscess. Hajare et al. and Weiss et al. generally reported more complications than our study [4, 9]. Regarding Eustachian tube function and mastoid pneumatization (E), our study revealed a high proportion of patients with E0 classification, indicating moderate to good pneumatization and ventilation. This finding differs from Hajare and Weiss et al., where most of the patients were classified as E2, suggesting a higher proportion of patients with sclerotic mastoids in their study population [4, 9]. Overall, while there are similarities in the distribution of some ChOLE subgroups across studies, differences exist, due to factors such as patient demographics, surgical techniques, and clinical practices on cholesteatoma classification and outcomes. Further research and comparative studies are necessary to better understand these variations and their implications for clinical management.
While the ChOLE Classification system offers a valuable framework for categorizing cholesteatomas, it is not without limitations. The classification fails to adequately represent every extent of cholesteatoma. Specifically, those that grow complicatingly medial to the ossicular chain, necessitating the degradation of individual ossicles, or those extending from the eardrum into the attic and further anteriorly into the anterior epitympanic recess or the tubal entrance, but not posteriorly toward the mastoid, are omitted. Additionally, cholesteatomas developing in the hypotympanum, particularly below the floor of the ear canal, are not accounted for.
Moreover, uncertainties exist within the “O” Category, such as the definition of a fixed stapes within stage O4a. In clinical practice, many stapes in chronic otitis media appear at least partially fixed. This distinction does not impact stages O0-O2, but it does alter stage O3a to O3b, prompting the question of why this alteration becomes relevant only when the fixed stapes is present alone, not as part of an intact ossicular chain. Furthermore, cases involving a fractured stapes footplate and rare instances where the malleus is absent but the incus is present are not addressed by the classification. Additionally, the significance of distinguishing between stages 4a and 4b is unclear, specifically regarding whether a fixed stapedial footplate still possesses a superstructure (O4a) or not (O4b). Moreover, isolated defects of the stapes superstructure, such as fractured or destroyed stapes legs due to cholesteatoma, cannot be classified.
Another critique concerns the category of “life-threatening complications” - the ‘L’ marking “life” implies severity, yet most of the listed extracranial complications are not life-threatening, particularly facial palsy, labyrinthine or semicircular canal fistulas, or labyrinthitis.
Unlike the other stages, determining the E stage is challenging to precisely define and the methodology is not entirely clear. Moreover, the distinctions between ventilation (possibly referring to “tubal function,” although gas exchange through the middle ear mucosa remains unaddressed) and pneumatization remain unclear. In such instances, classification with the ChOLE classification becomes impractical. Furthermore, the classification was partially limited due to a lack of detailed description of the respective pathology in the surgical report. In the future, aligning descriptions in the surgical reports with the classification will enhance the precision of the classification. For instance, the assessment of Eustachian tube ventilation was often unavailable as it was not documented in the surgical report, and imaging was frequently absent. A further potential limitation of this study is the retrospective design.
The ChOLE classification was primarily developed to illustrate the extent of destruction from surgical perspectives. However, it fails to depict the surgical effort involved in eradicating the cholesteatoma and especially in reconstructing the ossicular chain. Yet, these factors precisely define the temporal, technical, and financial resources required, and thus should be integral parts of a meaningful classification aimed at facilitating triage within a DRG system.
A limitation of this study is that while short-term outcomes, such as surgical duration, offer insights into immediate recovery, they may not reliably predict the long-term course of illness. Broader factors, such as patient health and the quality of follow-up care, are more critical in ensuring long-term safety. Focusing solely on surgical duration risks overlooking essential elements of recovery, as its effectiveness in warranting long-term patient safety is limited. Therefore, short-term outcomes should be considered alongside other factors to provide a more accurate assessment of long-term health outcomes.
In summary, these findings suggest that the ChOLE classification system can provide valuable insights into the complexity of cholesteatoma cases and their impact on duration of surgery. Understanding these correlations can help surgeons better anticipate surgical challenges, tailor treatment strategies, and optimize patient care in cholesteatoma management. Further research and validation of these findings could enhance surgical decision-making and improve patient outcomes in cholesteatoma surgery.



留言 (0)