Ethical approval
The study was ethically approved by the Medical Research Involving Human Subjects Act of the Maastricht University Medical Center + (MUMC +) and Maastricht University (UM) (NL66835.068.18/METC 18–040) and registered prospectively in the Dutch Trial Register (CCMO Onderzoek met mensen, https://onderzoekmetmensen.nl/nl/trial/56176).
Study design
This prospective cohort follow-up study was part of the Multidisciplinary Research on Repeated Implantation Failure and Recurrent Miscarriages (MURIM) study. The study protocol has been published before [19]. Briefly, the MURIM study analyses the steroid profile, microbiome and immunology status in patients with RIF, recurrent miscarriages and fertile controls. Female patients visited the RIF outpatient clinic during the window of implantation, 5 to 8 days after a positive ovulation test. The visit included a questionnaire, BMI and blood pressure measurement, an endometrial biopsy (“scratch”), a vaginal ultrasound, the collection of vaginal mucus and peripheral blood. Primary infertility was defined as never having conceived before. Systolic blood pressure > 140 mmHg and/or diastolic blood pressure > 90 mmHg was considered as hypertension. The vaginal mucus was used to determine the vaginal microbiome via the ReceptIVFity test. The ReceptIVFity test is a predictive test to assess an individual’s suitability for embryo implantation based on the microbiome resulting in a low, medium or high profile in the upcoming two months [20]. The blood sample was used to determine hormone (oestradiol, progesterone, free thyroxine (fT4) and thyroid stimulating hormone (TSH)) and vitamin D levels. After visiting the RIF outpatient clinic, patients were followed up for 1 year to monitor subsequent fertility treatments as well as occurrence and outcome of pregnancy. Although treatment advices were given, the ability of the RIF outpatient clinic to improve pregnancy chance and increase the number of patients who elected to continue with treatment was beyond the scope of this study.
Study participants
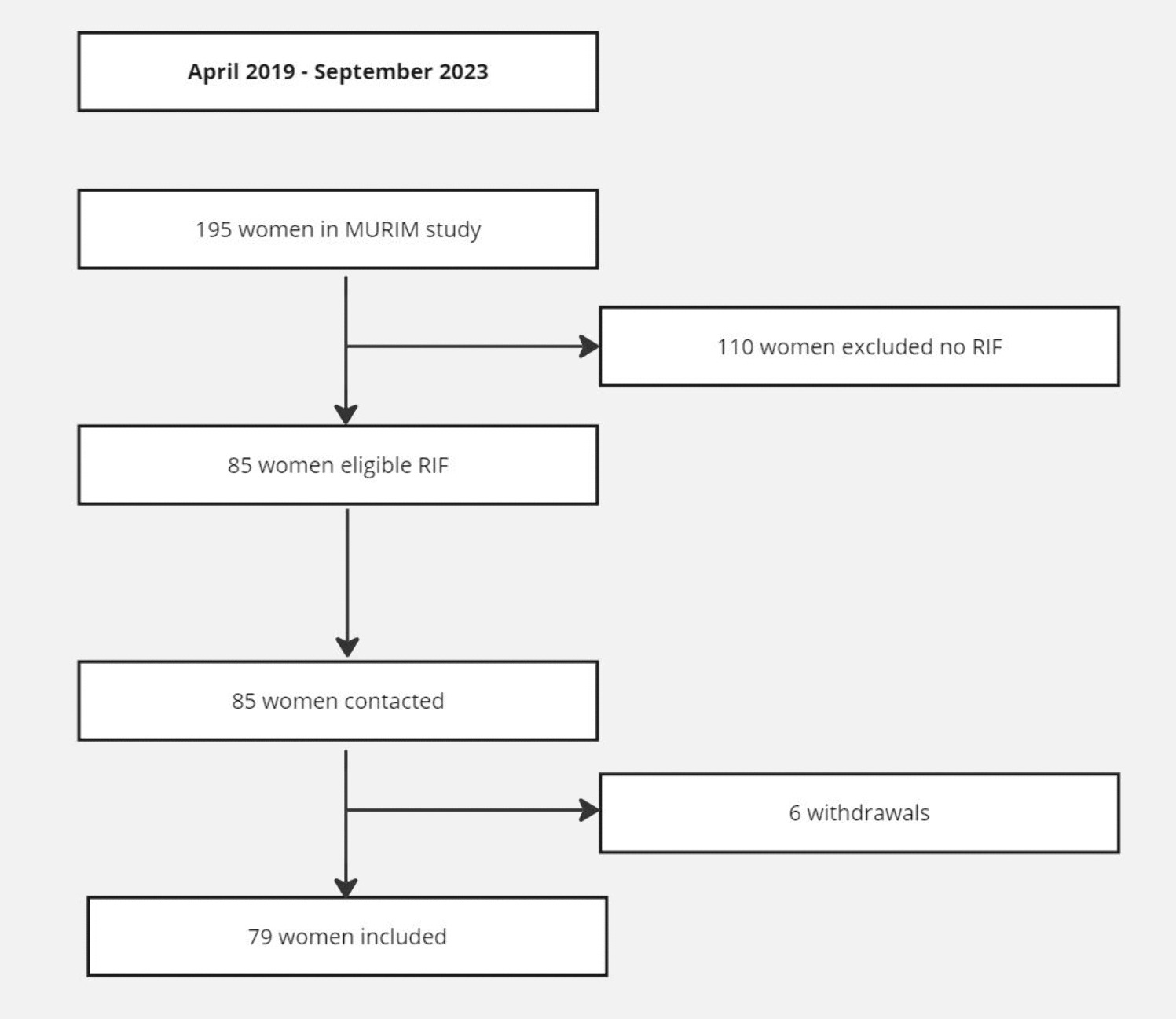
All IVF patients who were referred to the RIF outpatient clinic and were included in the MURIM study during the time period of April 2019 until September 2023 were selected as part of this follow-up study. The RIF group consisted of patients aged between 18 and 38 years old who were treated at the MUMC + or elsewhere in the Netherlands and were referred to the MUMC + for RIF. RIF was defined as implantation failure after three transfers of high-quality embryos or after transfer of ten or more embryos in multiple transfers [7]. High-quality embryos were defined using Gardner criteria. High quality was defined as (i) cleavage-stage embryos consisting of 4-cells (2 days following fertilization) or ≥ 7 cells (3 days following fertilization) both with less than 20% fragmentation and the absence of multinucleation, (ii) 4 days following fertilization: morula grade A or blastocyst grade B1 or B2, (iii) 5 or 6 days following fertilization: blastocyst grade B3 or more combined with inner cell mass quality A or B and trophectoderm epithelium quality A or B. Exclusion criteria for RIF were BMI > 35 kg/m2, clinically relevant intrauterine pathology, untreated endocrine abnormalities or pre-implantation genetic testing (PGT) treatment for monogenetic disorders or structural rearrangements (PGT-M or PGT-SR). PGT for aneuploidy (PGT-A) is not performed in the Netherlands because of the current legislation, so aneuploidy data of the embryos of the included patients were unknown.
Informed consent regarding a 1-year follow-up was obtained at the start of the MURIM study. Participants consented to receive a questionnaire and/or to have the medical file examined.
RIF diagnosis and treatment
After visiting the RIF outpatient clinic, treatment advices were given based upon the clinical outcomes. Lifestyle advices were given in case of smoking, alcohol abuses or high caffeine intake (> 200 mg per day). Weight loss and physical activity were advised in case of a high BMI (> 25 kg/m2). If the endometrium was thin (< 7 mm) during the WOI, it was advised to monitor endometrial thickness with an ultrasound before the next embryo transfer. If the endometrium remained thin, it was advised to change treatment protocol (e.g. artificial frozen cycle with oestradiol to natural cycle or natural cycle to artificial frozen cycle with follicle stimulating hormone) to potentially increase endometrial thickness. If vitamin D was low (< 50 nmol/L), supplements (10 mcg vitamin D/day) were advised. In case of low progesterone (< 20 nmol/L), progesterone supplements were advised when cryopreserved embryos were transferred in a natural cycle. In case of thyroid dysfunction, patients were referred to their general practitioner for treatment. When the ReceptIVFity outcome was low, treatment was delayed with three months. The ReceptIVFity test was repeated after 3 months but even in case of another low profile the IVF attempt was resumed, as no treatment was available yet.
Instruments and data collection
A questionnaire was used to obtain relevant information from the study participants. The questionnaire elicited information regarding (dis)continuation of fertility treatment after participation in the MURIM study as well as occurrence of ongoing pregnancy during the 1-year follow-up period. The eligible patients were invited to participate 1 year after their visit to the outpatient clinic to participate in the study and were sent a short questionnaire on paper or by email. Missing information was collected via medical files and patients were called if there was no reply by post or email. Clinical factors obtained at intake at the RIF outpatient clinic were used as baseline characteristics. Missing data is reported and not imputed.
Control group and ESHRE working group definition
To compare cumulative ongoing pregnancy rate in IVF women with RIF with non-RIF patients, the centre-specific treatment-process planning tool was used to determine all eligible IVF patients that could be included in the control group. All patients who started their first IVF or ICSI treatment at the MUMC + between January 2022 and April 2023 were analysed until data of 100 patients was gathered. Patients were included in the control group if they were between 18 and 38 years old and had a BMI < 35 kg/m2. Then, 1:1 matched controls were selected, matched for age, primary vs. secondary infertility and BMI. At last, indication for the IVF/ICSI treatment, duration of infertility, amount of ETs in the follow-up period and ongoing pregnancy rate was determined in the first year after the start of their first attempt via their electronic patient file.
To compare how many of the included RIF patients complied with the recommendations on RIF that were proposed by the ESHRE Working Group in 2023 [21], we used the recommended threshold of 60% predicted cumulative chance of implantation to identify RIF as defined by the working group based on the European IVF Monitoring Programme data [22].
Statistical analysis
The primary outcome measures were incidence of ongoing pregnancy and time to pregnancy within 1 year after participation in the MURIM study. Time to pregnancy was calculated as time in months between visiting the RIF outpatient clinic and the date of the first positive pregnancy test which eventually led to a pregnancy lasting at least 12 weeks. Secondary outcome measures were (i) amount of embryo transfers to achieve ongoing pregnancy within one year after visiting the RIF outpatient clinic (“transfers to pregnancy”), (ii) method of conception (fresh or frozen embryo transfer), (iii) pregnancy outcomes and (iv) influence of baseline determinants on pregnancy chance. Normal distribution of baseline characteristics was assumed based on the amount of participants [23]. Baseline characteristics were compared between patients who did and did not achieve ongoing pregnancy within the 1-year follow-up period using univariable analysis. Continuous variables were compared using an independent Student’s T-test. For categorical variables, risk ratios (RR) were calculated to compare exposure in non-pregnant vs. pregnant patients using OpenEpi version 3.01 (www.OpenEpi.com). The Statistical Package for the Social Sciences (SPSS v 22 for Windows, Chicago, IL, USA) was also used for data analysis. A p-value below 0.05 was considered statistically significant. Data are presented as mean (± SD) or number (%). Time to pregnancy is shown as median values with interquartile range (IQR). Transfers to pregnancy are presented as mean with 95% confidence intervals (CI).
Time to pregnancy and number of transfers to pregnancy were estimated by one minus Kaplan–Meier (KM) survival curves. Time to pregnancy does not take into account that couples might choose for a break in their treatment and have very little chances during that month (as spontaneous pregnancy chances in RIF patients are assumed to be low). Therefore, embryo transfers to pregnancy are calculated as they are more informative in a clinical setting. Censoring of data was applied in two different ways to determine transfer to pregnancy survival curves. Typically, in KM curves, patients are censored if they stop further treatment during the follow-up period (“optimistic curve”). In the optimistic scenario, it is assumed that patients who stopped treatment had the same probability of achieving an ongoing pregnancy after IVF/ICSI as those who continued. However, to avoid overestimation of pregnancy chances, a second curve was calculated (“pessimistic curve”) which accounts for the scenario that the participant who stopped treatment was advised to do so because of a poor prognosis. The pessimistic curve assumes that patients who stopped treatment without achieving pregnancy had no more chance of achieving pregnancy [24]. In this scenario, the amount of patients at risk during the embryo transfer was used to calculate the cumulative incidence of ongoing pregnancy for all subsequent embryo transfers, regardless of the reason why they stopped further treatment. The transfer could have either implied a transfer of one or two embryos.






留言 (0)