Population
For this study TGA patients after ASO aged 8 to 40 years were prospectively recruited between December 2018 and September 2020. Exclusion criteria included presence of a stent in the pulmonary arteries, presence of a cardiac pacemaker and all contra-indications for CMR including claustrophobia and pregnancy. Patients underwent CMR according to the routine TGA protocol (including cine images) of our centre, with the addition of 4D flow CMR. Routine echocardiography was preferably performed on the same day of CMR. Written informed consent was obtained for all patients and/or their guardians (for patients < 16 years of age). This study was approved by the local Medical Ethical Committee (Study Number 18-200).
CMR Acquisition
CMR imaging was performed on a 3.0 Tesla scanner (Ingenia R5.6.1, Philips Healthcare, Best, The Netherlands). Velocity encoded 2D PCMR scans with ECG-triggering and a single breath-hold were acquired for the main PA (MPA), left PA (LPA) and right PA (RPA). The plane was positioned at the site where the vessel diameter was considered smallest, which was assessed visually on axial and coronal views. Imaging parameters for the 2D PCMR were as follows: spatial resolution = 1.25 × 1.25 mm2, FOV = 320 × 320 mm2, slice thickness: 5 mm, number of cardiac phases: 25, echo time = 2.8–3.4 ms, repetition time = 4.9–5.5 ms, flip angle = 10°, bandwith = 479 Hz/pixel, venc = 180–350 cm/s. Scan times were typically around one minute per scan. All scans were checked for velocity-aliasing directly after the end of each scan and repeated with altered venc if necessary.
4D flow CMR acquisition was performed with prospective ECG and respiratory navigator-gating. The acquired volume covered the entire MPA, LPA and RPA. Imaging parameters for the 4D flow CMR were as follows: spatial resolution = 2.5 × 2.5 × 2.5 mm3, FOV = 300 × 300–350 × 350 mm2, temporal resolution = 32.8–46,1 ms, echo time = 2.1–2.5 ms, repetition time = 3.9–4.5 ms, flip angle = 10°, venc = 200–450 cm/s, TFE factor 3, SENSE: 2.5 (AP) and 1.5 (RL). Concomitant gradient correction and local phase correction was performed from standard available scanner software. Scan times were typically 8–12 min per scan.
CMR Post Processing
Post processing for 2D PCMR acquisitions was performed with 2D PCMR software (CAAS MR Solutions, version 5.0-5.1, Pie Medical Imaging, Maastricht, the Netherlands). The region of interest was manually segmented by one observer (EW). From these regions of interest, peak velocity, forward flow and regurgitant flow were collected. Stroke volume was defined as forward flow–regurgitant flow and calculated for the MPA, LPA, and RPA.
4D flow CMR data was pre-processed using automatic background and velocity aliasing correction (CAAS MR Solutions, version 5.0-5.1, Pie Medical Imaging, Maastricht, the Netherlands). If aliasing artefacts could not be corrected, patients were excluded from this study. In case of minimal aliasing (defined as one or two voxels) the measurements were performed in the next plane without artefacts. Segmentation of the vessel was performed automatically and subsequent manual correction was done by a single observer with two years of experience in arterial segmentation of 4D flow CMR scans (EW). Regions with the maximum velocity were determined by retrospectively placement of 2D planes at the site where the maximum velocity was suspected, which was determined visually using color-coded streamlines visualization and velocity overlay for the region of interest within the plane. The plane was repositioned until the region with the maximum velocity was identified. From the regions of interest, peak velocity, forward flow and regurgitant flow were collected and stroke volumes were calculated. Aliasing correction was validated using flow mapping in a region proximal and distal to the plane and comparing the flows to the flow in the plane of interest.
Echocardiography
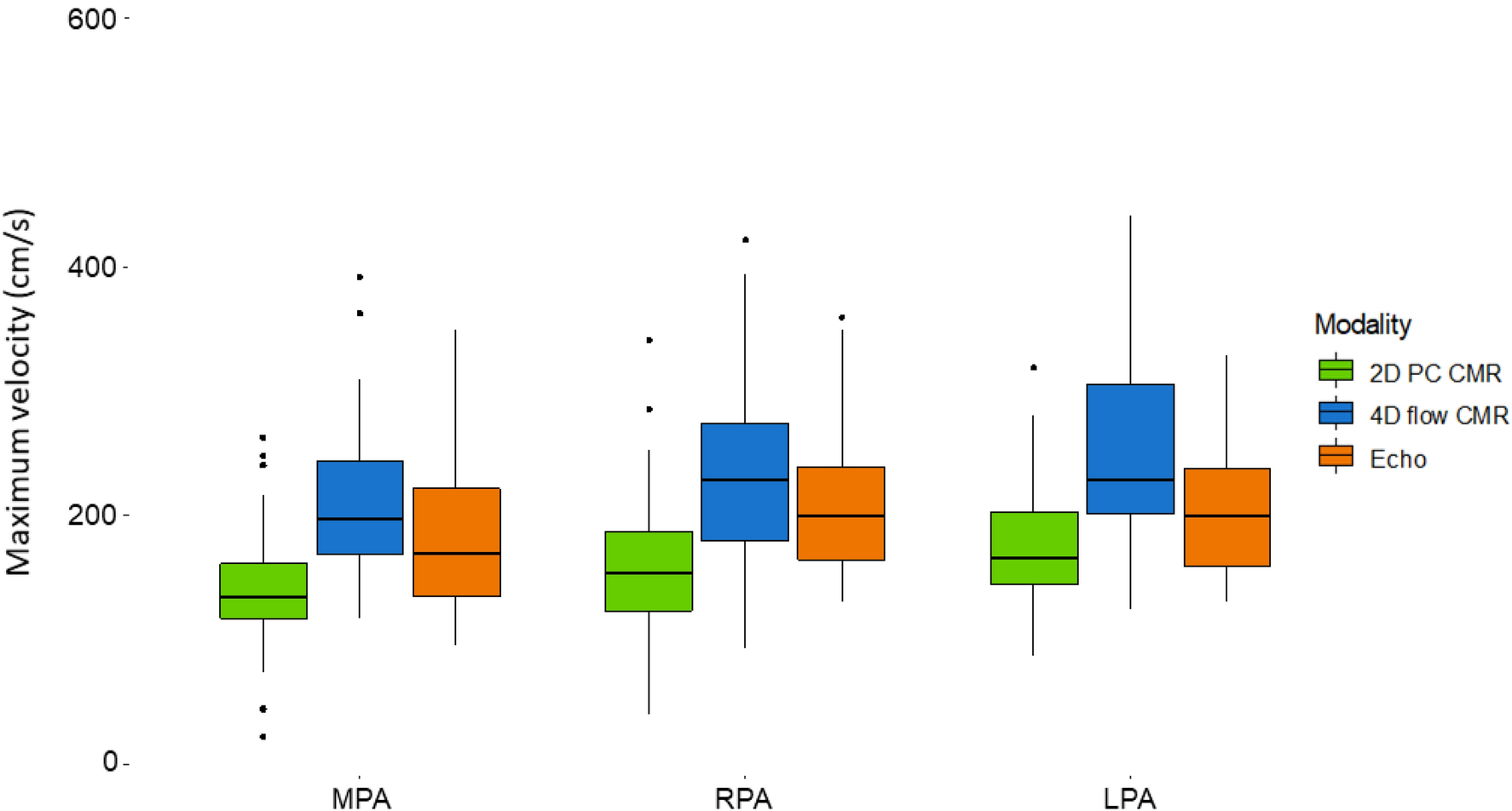
Echocardiography was performed by an experienced cardiac sonographer using General Electric (GE Healthcare, Wauwatosa, Wisconsin, USA) ultrasound systems, using the optimal transducer for patient size. Parameters collected for this study were maximum instantaneous velocities from Doppler images for the MPA, LPA and RPA.
Statistical Analyses
Statistical analysis was performed using R version 3.6.3 [8], and figures were produced using the package ggplot2 [9]. All data were assessed for normality using histograms, QQ-plots and the Shapiro–Wilk test. The paired Student’s T-test or Wilcoxon matched-paired signed rank test was used to compare measurements from the different modalities, depending on data distribution (normal or non-normal). Agreement between the different modalities was assessed using Bland–Altman analyses. To assess the proportion of patients with PS in our cohort, we dichotomized patients into two groups based on the peak velocities measured in the RPA and LPA. A peak velocity > 250 cm/s was classified as clinically relevant PS; a lower peak velocity was considered to be normal. The significance level was set at 0.05.








留言 (0)