
記住我

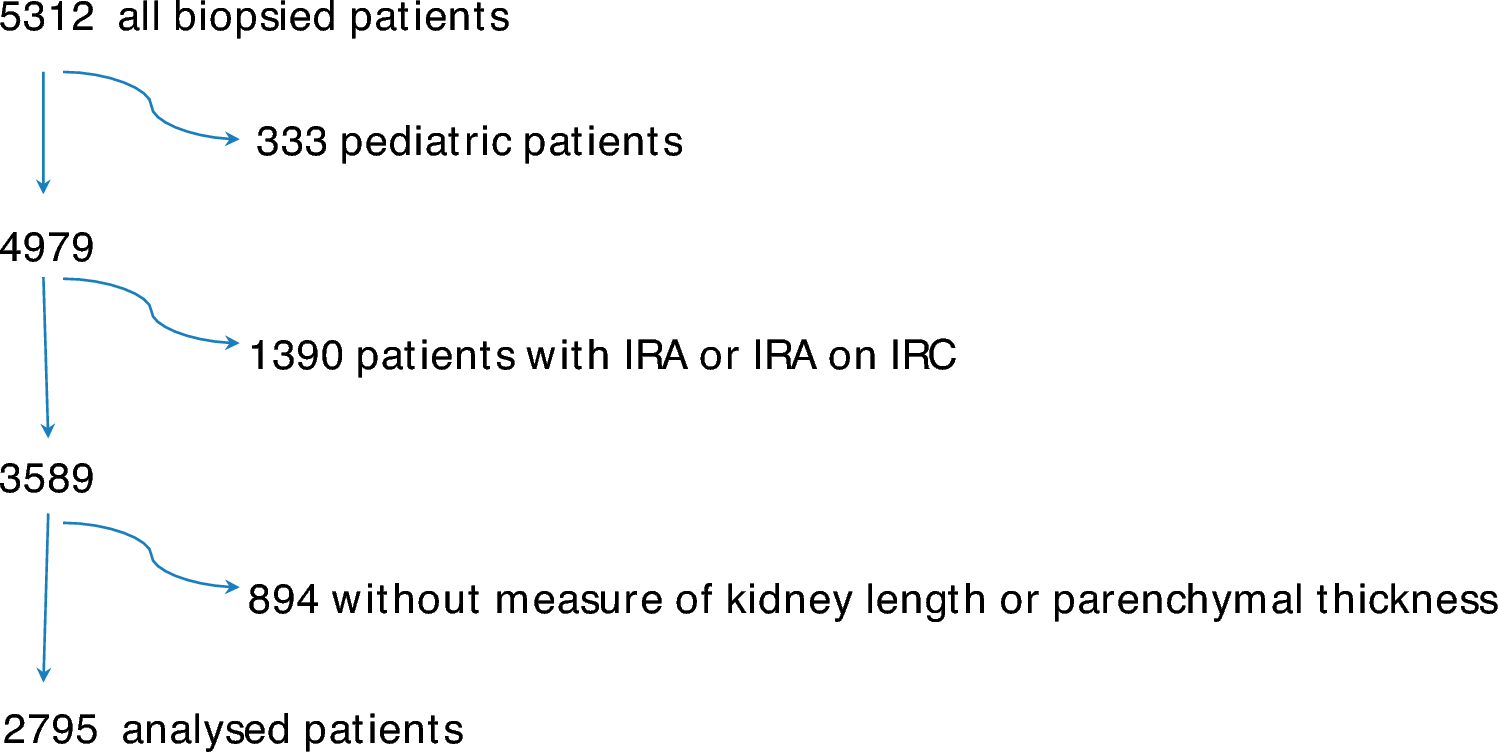
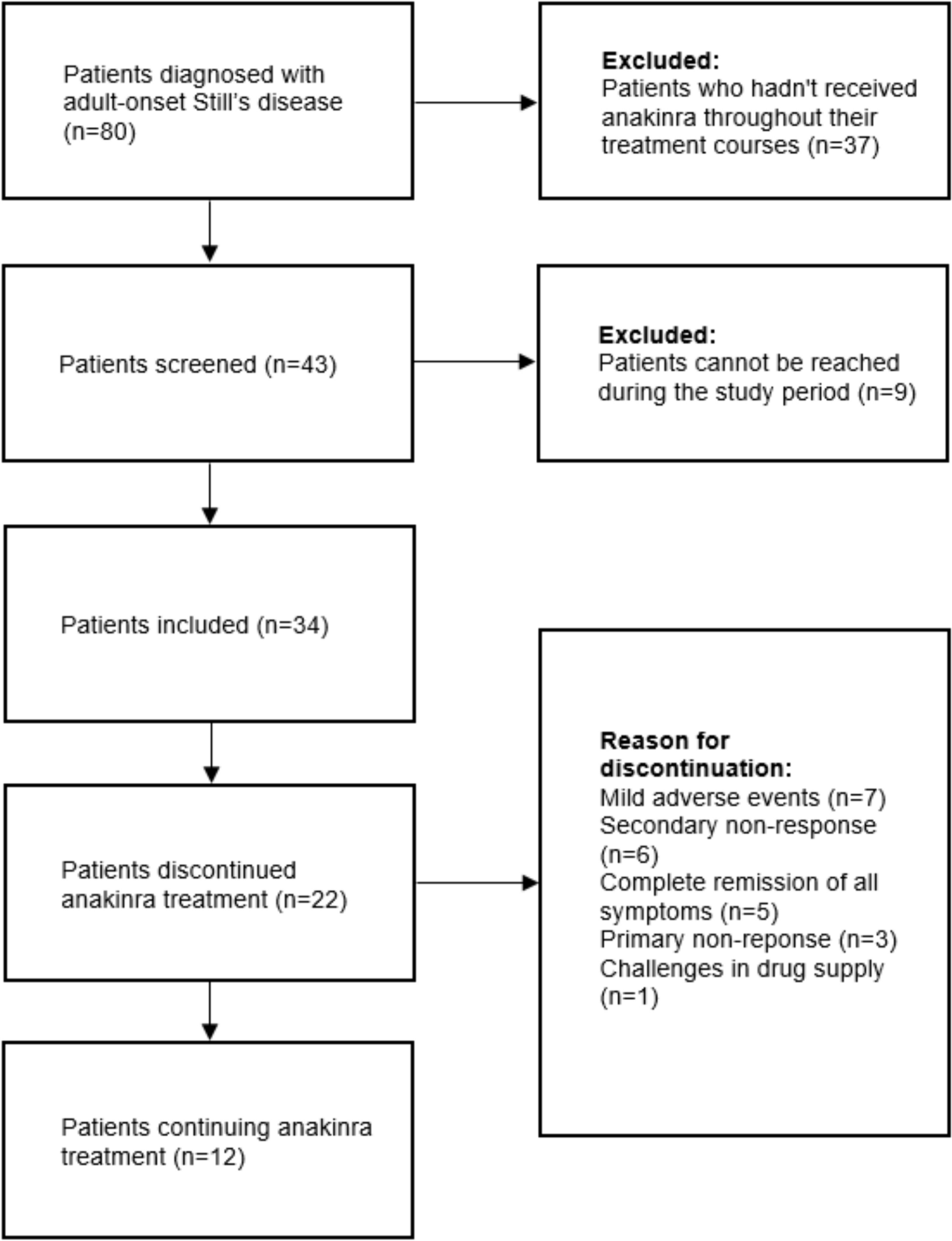
Our study identified 429 consecutive patients receiving liver transplantation. After chart review, we excluded 63 patients with transplant surgery due to acute liver failure and no previous history of chronic liver failure, patients not undergoing their first LT (i.e. reoperation) and any combined transplantation (concomitant kidney or heart transplantations). High-trauma fractures (motor vehicle accidents, etc.) were not counted as fragility fractures. All the remaining fractures were considered to be due to low-trauma or osteoporosis, unless otherwise stated. Twenty-six patients (6.0% of the total cohort) had missing or inaccessible radiological imaging/reports and were also excluded. A total of 366 patients were included in the final analysis (Figure S1, supplementary).
Characteristics of liver transplant recipients: whole population and gender comparisonOf 366 LT recipients included in the study, the majority of them had viral cirrhosis—144 (39.3%)—and 94 (25.7%) had multifactorial disease (Table 1 and 2). Of the 94 patients with multifactorial disease, 61 (64.8%) had viral + alcoholic etiologies, 14 (14.9%) had viral + rare disease etiologies, 13 (13.8%) had viral + MASH etiologies, 1 (1.1%) had cholestatic + viral etiologies, 3 (3.2%) had viral + alcoholic + MASH etiologies, and 2 (2.1%) had alcoholic + MASH etiologies. The overall cohort was composed of 107 (29.3%) women and 259 (70.7%) men, with significant differences in sex prevalence among the etiology categories, with autoimmune and cholestatic disease being more prevalent in women (9.3% and 10.3% vs. 0.1% and 4.2%, respectively), while ALD and multifactorial disease being more common in men (13.9% and 28.6% in men vs. 5.6% and 18.7% in women, respectively). Clinical and anthropometric characteristics are shown in Table 1 and 2. The mean age was 52 years with no significant difference between women and men. A positive smoking history was more frequent in men (26.6% vs. 10.3%, P = 0.001). Diabetes and hepatocellular carcinoma were more frequent in men than in women, while females were more frequently exposed to glucocorticoids. Mean body mass index (BMI) was 25.6 kg/m2, with no differences between sexes. Hip BMD and estimated glomerular filtration rate (eGFR) were lower in women than in men, while hypertension was similar between the sexes (Table 1 and 2).
Table 1 Clinical characteristics of the whole population, according to sex: continuous variablesTable 2 Clinical characteristics of the whole population, according to sex: categorical variablesInstead, when we compared patients without fractures (84/211) versus patients with fractures (65/155) no differences occurred about the presence of hepatocellular carcinoma in the two populations (P 0.683).
Regarding bone metabolism, fragility fractures prevalence was 155/366 (42.3%) in the overall population, with no significant differences between sexes (fracture prevalence in women was 37.4%, in men was 44.4%). Calcium and vitamin D3 supplements were equally distributed among both sexes, while a small proportion of patients were taking bisphosphonates (13/366, 3.5%). Laboratory parameters of mineral metabolism were tested in very few patients, and no significant differences could be observed between sexes.
Among patients with vertebral fractures (n = 145), mild vertebral fractures (Genant grade 1) were the most frequently observed (90/145, 62.1%), with similar prevalence between sexes. Moderate vertebral fractures (Genant grade 2) were more common in men compared to women (33.9% vs 16.7%, P < 0.05). Severe (Genant grade 3) vertebral fractures occurred more frequently in women compared to men (16.7% vs. 5.5%, P < 0.05). The overall number of patients with clinical fragility fractures (i.e. symptomatic) was 50/366 (13.7%). Of these, most (n = 43, 86%) were vertebral fractures. Other clinical fractures were at the humerus (n = 1), ribs (n = 7), femur (n = 1), and clavicle (n = 1). The median time between clinical fracture occurrence and LT was 2 months. All the remaining fractures were morphometric vertebral fractures. Fracture prevalence among transplant recipients was stable across each year of the study period (Figure S2, supplementary).
Women with fractures, compared to women without fractures had worse kidney function, lower urinary calcium, lower BMD and more commonly having alcoholic etiology (Supplementary Table a. and b.). Compared to men without fractures, men with fractures had lower 25-OH vitamin D levels, with no other noticeable significant differences in laboratory or clinical data (Supplementary Table c. and d.).
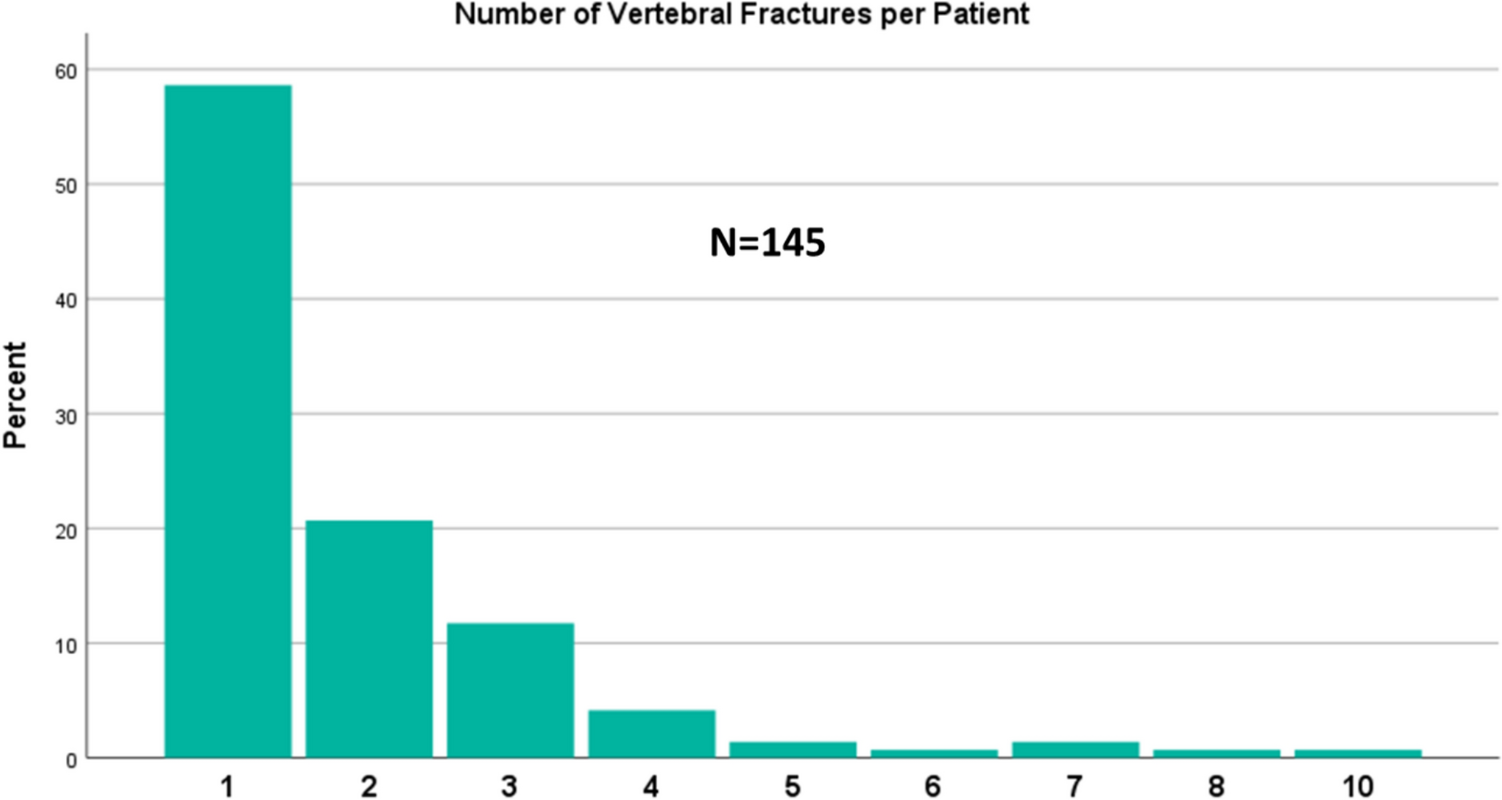
Most vertebral fractures were single fractures, although a significant proportion of patients (n = 60, 41.3%) had two or more vertebral fractures, up to a maximum of 10 vertebral fractures per patient (Fig. 1).
Fig. 1
Distribution of single and multiple vertebral fractures across patients with vertebral fractures (N = 145)
Characteristics of liver transplant recipients with bone fracturesPatients with bone fractures presented similar age and BMI compared to patients without fractures, although serum glutamic pyruvic transaminase (GPT) was lower and serum creatinine greater than patients with no fractures. Other parameters, both from clinical history and laboratory, were similar between groups (Table 3 and 4). The severity of liver disease was not different between groups. Fragility fractures showed similar rates across each liver disease etiology (Figure S3, supplementary). The most common vertebral sites were at T7, T8, T9 and T12 vertebrae (Fig. 2). Lower rates of fractures were observed in the lumbar spine. The most frequently observed vertebral fracture type was wedge fractures, with a minor but significant proportion of crush or biconcave fractures (Figure S4, supplementary).
Table 3 Clinical characteristics of the patients with and without fractures: continuous variablesTable 4 Clinical characteristics of the patients with and without fractures: categorical variablesFig. 2
Distribution of vertebral fractures (absolute frequencies)
Characteristics of liver transplant recipients: effect of glucocorticoids on metabolic bone diseaseGlucocorticoid administration differed across etiologies, although its impact on fragility fractures, vertebral fractures, or bone mineral density by DXA was not evident (Supplementary Table e.).
Characteristics of liver transplant recipients: effect of diabetes on metabolic bone diseaseDiabetes prevalence differed according to etiology, although it was not associated with fragility fractures (P = 0.192), vertebral fractures prevalence or severity, or low bone density by DXA (Supplementary Table f.).
Predictors of bone fragility fracturesA logistic regression model including age, sex, BMI, alcohol use, eGFR, etiology (autoimmune or cholestatic disease vs. other), revealed that only BMI was negatively associated with prevalent fragility fractures (odds ratio, OR 1.058, 95% CI 1.001–1.118, P = 0.046), independent of other risk factors. In LT recipients, for each one-unit decrease of BMI, the risk of fragility fractures would increase by 5.8%, and vice versa (Table 5).
Table 5 Multinomial logistic regressiona
留言 (0)