
記住我








Gallbladder cysts are rare diseases with very few reported cases, and no clinical or histological definition has been established. The cause of gallbladder cysts is thought to be that some trigger blocks the communication between the RAS and the gallbladder lumen, causing the RAS to expand within the gallbladder wall and form a cyst, but the details are not clear [1, 2]. Furthermore, cases of giant cysts outside the gallbladder wall are extremely rare.
Herein, we present a very rare case of giant gallbladder cyst with acute cholecystitis revealed by cholecystectomy after PTGBD.
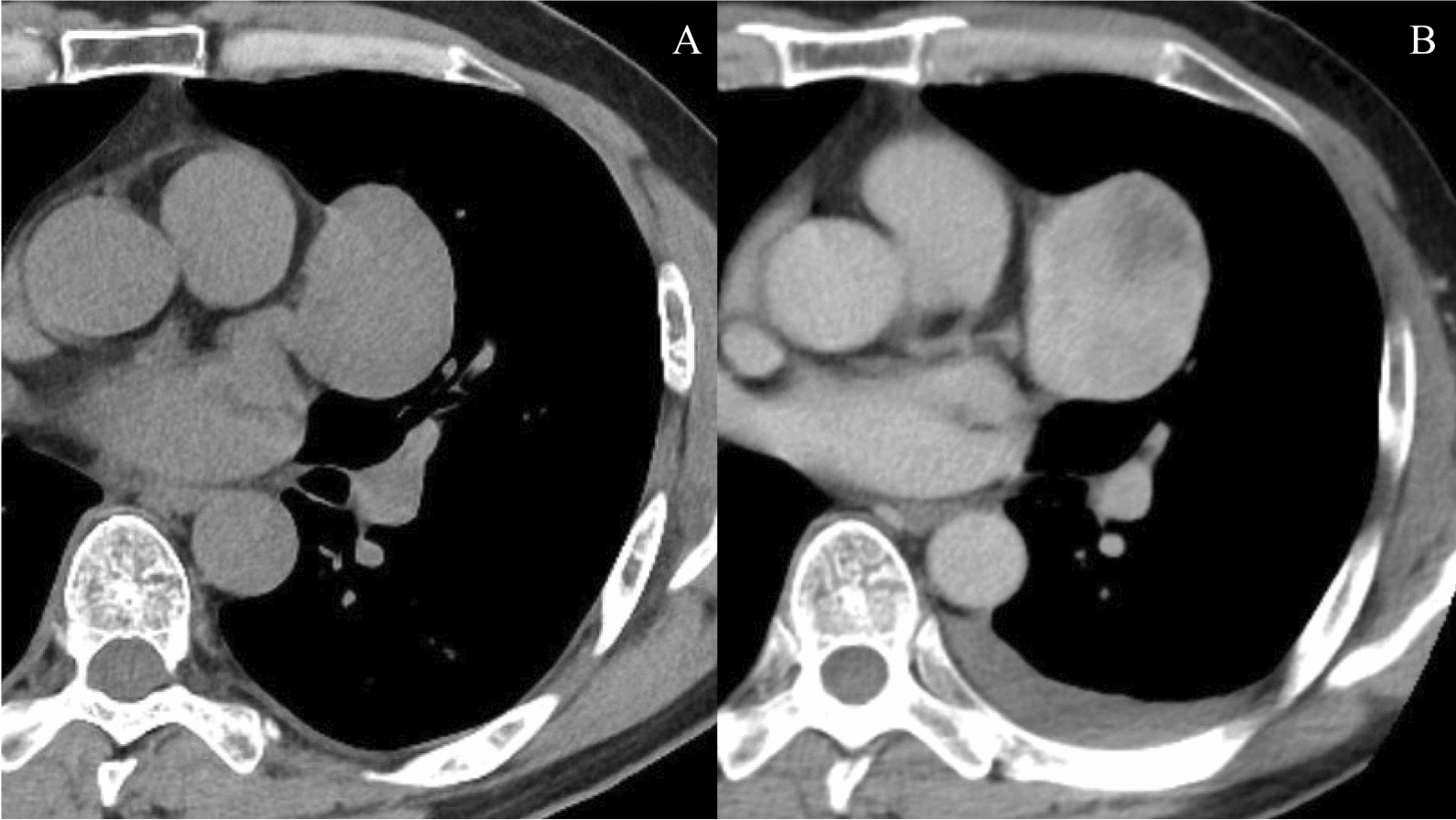
Case presentationAn 85-year-old woman with appetite loss and right lower abdominal pain lasting 2 days presented to our hospital. At first, the patient’s abdominal pain was mild to moderate with no fever. Blood tests revealed a white blood cell count of 10,950/mm3 and a CRP level of 14.35 mg/dl. Total bilirubin, indirect bilirubin, aspartate aminotransferase (AST), alanine transaminase (ALT), and alkaline phosphatase (ALP) were increased (3.5 mg/dl, 3.2 mg/dl, 99 U/l, 97 U/l, and 192 U/l, respectively). There was a mild increase in serum carcinoembryonic antigen (5.7 ng/ml) and a normal level of carbohydrate antigen 19–9 (21.1 ng/ml) (Table 1). Abdominal ultrasound sonography revealed a large cystic tumor in the right upper quadrant to lower quadrant with edematous wall thickness, fluid correction and a stone without a tumorous lesion, suggesting an enlarged gallbladder. A contrast-enhanced CT scan of the abdomen revealed a grossly distended gallbladder (14.5 × 14.5 × 8.7 cm) containing stone. CT scan also revealed significant gallbladder wall thickness and increased density of the surrounding adipose tissue, suggesting acute cholecystitis. In addition, impaction of a stone in the cystic duct, which was compressed to dorsal side, was suspected (Fig. 1).
Table 1 Laboratory data on admissionFig. 1
A contrast-enhanced CT scan of the abdomen revealed a grossly distended gallbladder (14.5 × 14.5 × 8.7 cm) containing a round stone (white arrow)
It was difficult to perform the operation at the time because of the grossly distended gallbladder. Then, the patient was treated via PTGBD. PTGBD was performed under US guidance. A pale-yellow, transparent, and serous drainage was observed. Drainage tube was determined to be within the gallbladder, and a 10 Fr drainage tube was placed (Fig. 2). The drainage volume was 735 ml.
Fig. 2
X-ray photograph showed the cavity after PTGBD insertion (white arrows)
MRCP revealed that gallbladder swelling had persisted (14.0 × 6.5 cm), and a stone remained in the gallbladder neck. MRCP also showed the V-shaped deformation of the extrahepatic bile duct with the gallbladder neck as the bending point suggested gallbladder torsion (Fig. 3).
Fig. 3
MRCP showed the V-shaped deformation of the extrahepatic bile duct with the gallbladder neck as the bending point (white arrow)
We performed laparoscopic cholecystectomy 6 days after PTGBD. Because of the severe adhesion around the junction of the cystic and common bile ducts, we performed a laparotomy (Fig. 4a). After removing the adhesions, we resected the gallbladder at the neck. We found no evidence of gallbladder torsion. The lesion was not a cystic lesion protruding from the liver but a cystic lesion associated with the gallbladder that had been dissected from the gallbladder bed during surgery (Fig. 4b).
Fig. 4
Surgical findings. Because of the severe adhesion around the junction of the cystic and common bile ducts, we performed a laparotomy (a). White arrows indicate a resected margin of the gallbladder and yellow arrows indicate the gallbladder bed (b)
The resected specimen was 14 × 11 cm in size and consisted of a gallbladder (6 × 7 cm) accompanied by a stone (2.4 × 1.8 cm) in the gallbladder and around a cystic lesion. The opened cystic lesion was 18 × 18 cm in size with gross wall thickness (6–12 mm) and contained pale yellow–reddish fluid (195 ml) accompanied by septal structures and purulent tissue inside the cavity. Macroscopically, there was no communication between the extramural cyst and the gallbladder lumen. There was no tumorous lesion (Fig. 5a, b). The patient’s postoperative course was uneventful, and she was discharged on postoperative Day 5.
Fig. 5
Macroscopic findings. The resected specimen was 14 × 11 cm in size and consisted of a gallbladder (6 × 7 cm) accompanied by a stone (2.4 × 1.8 cm) and around a cystic lesion (a, b). White arrows indicate the gallbladder and yellow arrows indicate the cystic lesions (a). The specimen shows the findings after the incision of an extramural cyst on the posterior side of the gallbladder (b)
Histopathological examination revealed infiltration of inflammatory cells, including neutrophils, in the gallbladder with no epithelial atypia (Fig. 6a, c), suggesting chronic cholecystitis accompanied by acute inflammation. The extramural cystic lesion showed a lamellar fibrin, and red blood cells in the lumen, and infiltration of lymphocytes, neutrophils, and eosinophils, with edematous wall thickness accompanied by proliferation of enlarged spindle cells (Fig. 6b, d). There was no malignancy (Fig. 6a–d). These findings suggested that both cholecystitis and cyst infection had occurred. A double gallbladder or a large diverticulum of the gallbladder was considered but could not be identified, because there was no epithelial component or smooth muscle layer in the wall of the cystic lesion.
Fig. 6
Histological findings of the resected specimen with HE staining. The specimen shows wall inflammation of the gallbladder wall (a) and wall thickness of the cystic lesion outside of the gallbladder wall (b). The specimen shows an infiltration of inflammatory cells, including neutrophils, in the gallbladder with no epithelial atypia (c). The specimen shows a lamellar fibrin, red blood cells in the lumen, and an infiltration of lymphocytes, neutrophils, and eosinophils in the wall of the cystic lesion. The thickened wall of the cystic lesion shows edema with proliferation of enlarged spindle cells (d). There was no malignancy (a–d)
留言 (0)