The study subjects comprised 989 adult women, who received genetic counselling and testing between 2011 and 2017 at the Clinical Hospitals of Pomeranian Medical University in Szczecin, Poland, or at an associated hospitals or outpatient clinics. At the first study visit, a fasting blood sample was collected from each study participant to be used for genetic testing for BRCA1 founder mutations. Within this cohort, 559 women had the c.5266dupC mutation, 250 had the c.181T/G mutation, 50 had c.4035delA, 18 had c.3700_3704delGTAAA, 14 had c.1687 C > T, 12 had c.5251 C > T, 9 had c.66_67delAG (or c.68_69delAG), and 9 had c.676delT; additionally, 68 women had other, less common mutations. For analysis, 10 mL of peripheral blood was collected into a vacutainer tube containing ethylenediaminetetraacetic acid (EDTA) from all study participants. All blood samples were collected between 8 a.m. and 2 p.m. and stored at − 80 ℃ until analysis. Participants were included in the study if a deleterious BRCA1 variant was detected. Typically, these patients are offered the opportunity to participate in other clinical research studies. Medical charts were reviewed for age of diagnosis, oral contraceptive use (ever/never), hormone replacement therapy use (ever/never), smoking history (yes/no), oophorectomy (yes/no). The study was conducted in accordance with the Helsinki Declaration and with the consent of the Ethics Committee of Pomeranian Medical University in Szczecin under the number KB-0012/73/10 of 21 June 2010. All participants provided written informed consent.
Measurement of blood molybdenum level
The blood samples were obtained from fasting individuals through venipuncture using the Vacutainer® System (BD #368381, Plymouth, UK). Blood was carefully divided into new cryovials and then frozen at -80 °C until analysis.
The elemental composition of the samples was determined using the inductively coupled plasma mass spectrometry (ICP-MS) technique with the NexION 350D instrument (PerkinElmer, Norfolk, USA). The KED (Kinetic Energy Discrimination) mode was employed for element determination, and rhodium was used as an internal standard to compensate for instrument drift and matrix effects. Detailed information regarding the specific parameters of the NexION 350D instrument used in the measurements can be provided upon request. During analysis, the blood samples were diluted 40-fold with blank reagent (70 µl blood: 2730 µl buffer).
The blank reagent used consisted of high-purity water (> 18 MΩ), tetramethylammonium hydroxide (TMAH) (AlfaAesar, Kandel, Germany), Triton X-100 (PerkinElmer, Shelton, CT, USA), EDTA (Merck, Darmstadt, Germany), and ethyl alcohol (Merck, Darmstadt, Germany).
Calibration curve standards were prepared by diluting the stock solution of 1000 µg/ml Molybdenum Standard (PerkinElmer Pure Plus, Shelton, CT, USA) with the blank reagent. The calibration method used was matrix matched, and the correlation coefficients for calibration curve was always greater than 0.999.
The accuracy and precision of the measurements were evaluated using certified reference materials (CRM): ClinChek® Plasmonorm Whole Blood Level 1 (Recipe, Munich, Germany) and Seronorm Whole Blood Level 2 (Sero, Norway). Technical details, plasma operating settings, and mass spectrometer acquisition parameters can be provided upon request. The testing laboratory participates in an independent external quality assessment scheme, QMEQAS (Quebec Multielement External Quality Assessment Scheme) organized by the Institut National de Santé Publique du Québec.
Statistical analysis
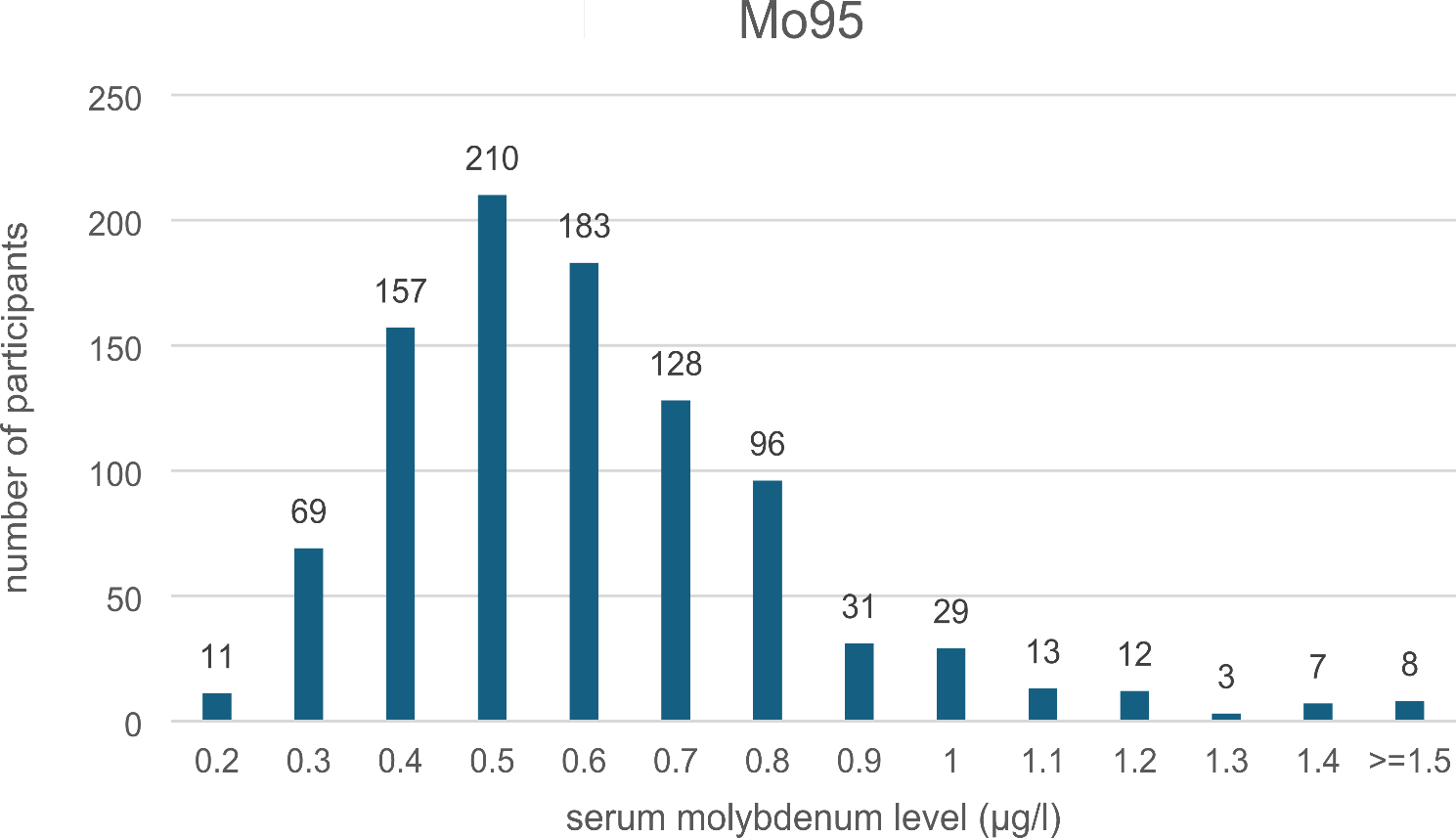
All study participants were assigned to one of three categories (tertiles) depending on their blood molybdenum level. The cumulative risks of breast and ovarian cancer were calculated from the age at blood draw to the age of diagnosis of breast or ovarian cancer, death from another cause, or last follow up. For estimating the risk of ovarian cancer, women with oophorectomy prior to blood draw were excluded and subjects with oophorectomy in the follow-up period were censored at the time of oophorectomy. For the analysis of breast cancer risk, oophorectomy was included as a time-dependent variable. To estimate the ten-year cumulative risk of ovarian cancer, patients were followed from blood draw to date of preventive oophorectomy, ovarian cancer, ten years of follow up, last follow up or death from another cause. In order to estimate the hazard ratios (HRs) for cancer risk, univariable and multivariable Cox proportional hazards regression analyses were performed. In multivariable models, the following variables were taken into analysis: molybdenum level (tertile), year of birth, age at blood draw (< 40 years, 40–49.9 years ≥ 50 years), oral contraceptive use (yes/no), hormone replacement therapy use (yes/no), smoking history (current, former never), BMI (< 23.0 versus > 23.0). All statistical analyses were performed using SAS, version 9.4.







留言 (0)