The EGFR T790M (c.2369 C > T) mutation leads to an amino acid change in exon 20 from threonine (T) to methionine (M). This mutation is found in 2% of lung cancers, with the germline form occurring in 1% of cases [19]. According to data from OrigiMed laboratory, the prevalence of EGFR T790M germline mutations in Chinese patients with NSCLC is lower than that observed in Japanese and American populations (0.08% vs. 0.54%) [17]. Preclinical studies have indicated that the T790M mutation increases EGFR kinase activity, thereby providing a mild proliferative impetus for lung cancer development [20]. Typically, lung cancers with T790M germline mutations are predominantly found in females, are mostly adenocarcinomas, and occasionally multifocal. Additionally, 73% of tumors with the T790M germline mutation also have other activating mutations in the EGFR gene. These findings are all consistent with our case report. We describe a male patient with lung adenocarcinoma who possessed the germline EGFR T790M mutation along with somatic mutations in EGFR 19-Del, TP53, and PIK3CA. This specific combination of mutations is extremely rare, with the first reported case of a patient having both germline EGFR T790M and somatic EGFR L858R and PIK3CA mutations documented by Lammers et al. [21].
EGFR T790M mutations are found in approximately 50% of patients who develop resistance to EGFR-TKIs, and these mutations are linked to acquired resistance to these therapies. Osimertinib, a third-generation EGFR TKI, effectively inhibits both EGFR TKI-sensitive and resistant EGFR T790M mutations in human NSCLC models. The US Food and Drug Administration (FDA) has approved Osimertinib for the treatment of metastatic NSCLC patients positive for the EGFR T790M mutation. Additionally, Osimertinib can be administered as a first-line treatment in patients with mutant EGFR lung cancer, either during initial EGFR TKI treatment or after disease progression [2, 22,23,24]. In our report, the proband achieved a 19-month progression-free survival using Osimertinib following postoperative progression of stage IV lung cancer. Subsequently, the patient was treated with targeted therapies including ameritinib and bevacizumab, ultimately extending survival to 42 months.
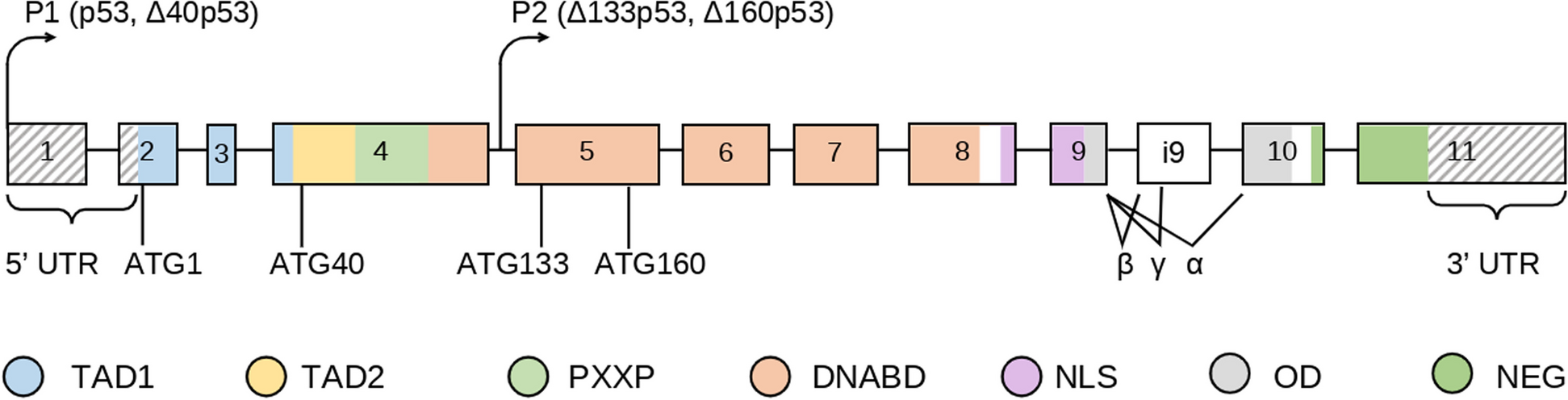
TP53 is the most commonly co-occurring mutation in NSCLC, with approximately 60% of patients harboring EGFR mutations also presenting TP53 mutations. These TP53 mutations are often linked to resistance against EGFR-TKIs in Chinese patients with NSCLC. TP53 mutations diminish the efficacy of TKIs in patients with EGFR-mutant NSCLC and are associated with a poorer prognosis, particularly for those with non-disruptive, non-missense mutations, and mutations outside the DNA-binding domain (DBD), specifically in exons 6 and 7. Thus, TP53 mutations serve as an independent predictor of outcomes in NSCLC patients treated with first-generation TKIs. Patients with both EGFR and TP53 mutations typically have a median progression-free survival (PFS) of only 6.5 months and a median overall survival (OS) of 28.0 months, nearly half that of controls [25, 26]. In our report, co-mutations of EGFR 19 Del, T790M and TP53 exon6 c.637 C > T p.(R213*) were detected in the tumor tissue of the proband. He achieved a PFS of approximately 19 months after treatment with the third-generation EGFR-TKI, Osimertinib, and an OS of 42 months. His prognosis exceeded those commonly reported in the literature.
Phosphoinositide 3-kinases (PI3Ks) play an important role in tumor development and progression, and recurrent activating mutations in the p110 α subunit (PIK3CA) have been found in some tumors. Several PI3K inhibitors have been approved for use in both solid tumors and hematological malignancies. The FDA has sanctioned the use of Alpelisib in combination with fulvestrant for treating HR+/HER2- advanced or metastatic breast cancer patients who have PIK3CA gene mutations [27]. In an elegant study reported by Lammers et al., a patient with both a germline EGFR T790M mutation and somatic EGFR L858R and PIK3CA mutations received a combination treatment of erlotinib 150 mg daily for four months, afatinib 40 mg daily, and cetuximab 500 mg/m2 bi-weekly for three months, along with a PI3K inhibitor for another three months. The patient maintained a good quality of life 23 months post-diagnosis of stage IV lung adenocarcinoma [21]. In our study, the PIK3CA exon10 c.1633G > A p.(E545K) mutation was found in the tumor tissue of the proband, but the mutation abundance was only 0.52%, so he was not treated with PIK3CA inhibitor. Unfortunately, Unfortunately, after disease progression following Osimertinib treatment, we were unable to obtain further tumor tissue for genetic analysis to identify changes in resistance genes. If the tumor presents with high mutation abundance PIK3CA mutations after Osimertinib resistance, patients will potentially benefit from PIK3CA inhibitor therapy [27].
When a patient exhibits more than two nodules, they are diagnosed with multiple ground-glass nodules (mGGNs), and these are classified as synchronous multiple primary lung cancer (SMPLC) when found in the lungs. With advancements in chest CT imaging technology, the incidence of mGGNs has risen sharply in recent years. mGGNs are more commonly observed in female non-smokers and may have a higher familial risk of malignancy compared to typical lung cancer patients [18, 28, 29]. In our study, the proband, who carried the EGFR T790M germline mutation, had multiple nodules in his left lung. Similarly, his two daughters, also carriers of the EGFR T790M germline mutation, showed multiple ground-glass density nodules in both lungs on their CT scans during a physical examination. Germline EGFR T790M mutations are exceptionally uncommon. For instance, none were found in a study involving 627 Japanese lung cancer patients [30, 31]. In a separate investigation among 31,906 Chinese lung cancer patients, only two instances of T790M germline mutations were identified. Among other EGFR germline mutations discovered, the G863D mutation was the most frequent, followed by P848L, D1014N, K757R, V897A, and R831H [32]. Thus, identifying these EGFR germline mutations is crucial for screening family members for potential cancer risks. Oxnard et al. recommended that any lung cancer patients with initial tumor tissue testing positive for EGFR T790M mutations should also have their peripheral blood samples retested to rule out the presence of germline mutations of EGFR T790M [33]. Although EGFR germline mutations are not typically included in routine screenings, there are several strategies to identify potential EGFR germline mutations during regular testing procedures. Firstly, it is crucial to thoroughly gather family history, especially of lung cancer, and perform EGFR and other germline gene tests for those patients who have a familial history. Secondly, the detection of specific mutations such as EGFR T790M, R776H, or V843I during pre-treatment genotyping for lung cancer may indicate a possible germline mutation. Finally, if repeated genetic tests on tumor tissue or peripheral blood ctDNA show a consistent mutation abundance of 50% for EGFR T790M, it is likely indicative of a germline mutation, and testing for EGFR germline mutations is recommended [10]. As mutation screening becomes more comprehensive and testing methods improve in sensitivity, an increasing number of patients are likely to be identified with suspected inherited or germline mutations. Crucially, these findings can impact not only the care of the patients but also their family members. Although there are no established guidelines for screening lung cancer in asymptomatic individuals with known EGFR germline mutations, it is recommended that family members who have been diagnosed with EGFR germline mutations undergo regular monitoring through CT scans.







留言 (0)