
記住我




A 62-year-old woman with no smoking history experienced itching on the left side of her chest 16 months before diagnosis. She visited a dermatologist, but no abnormality was found, and she was followed up with. Seven months later, she fell and bruised her chest. Since then, she had left-sided chest pain when coughing and sneezing. She was prescribed painkillers, but the left-sided chest pain gradually became more severe. She thought it was caused by yoga, which she had recently started practicing. She visited a general practitioner who noted multiple masses in both breasts.
Her only medical history was of scoliosis and chronic gastritis, neither of which required treatment.
She had no family history of cancer, no allergies, no alcohol consumption, or no smoking.
A screening mammogram 6 months earlier revealed no abnormalities.
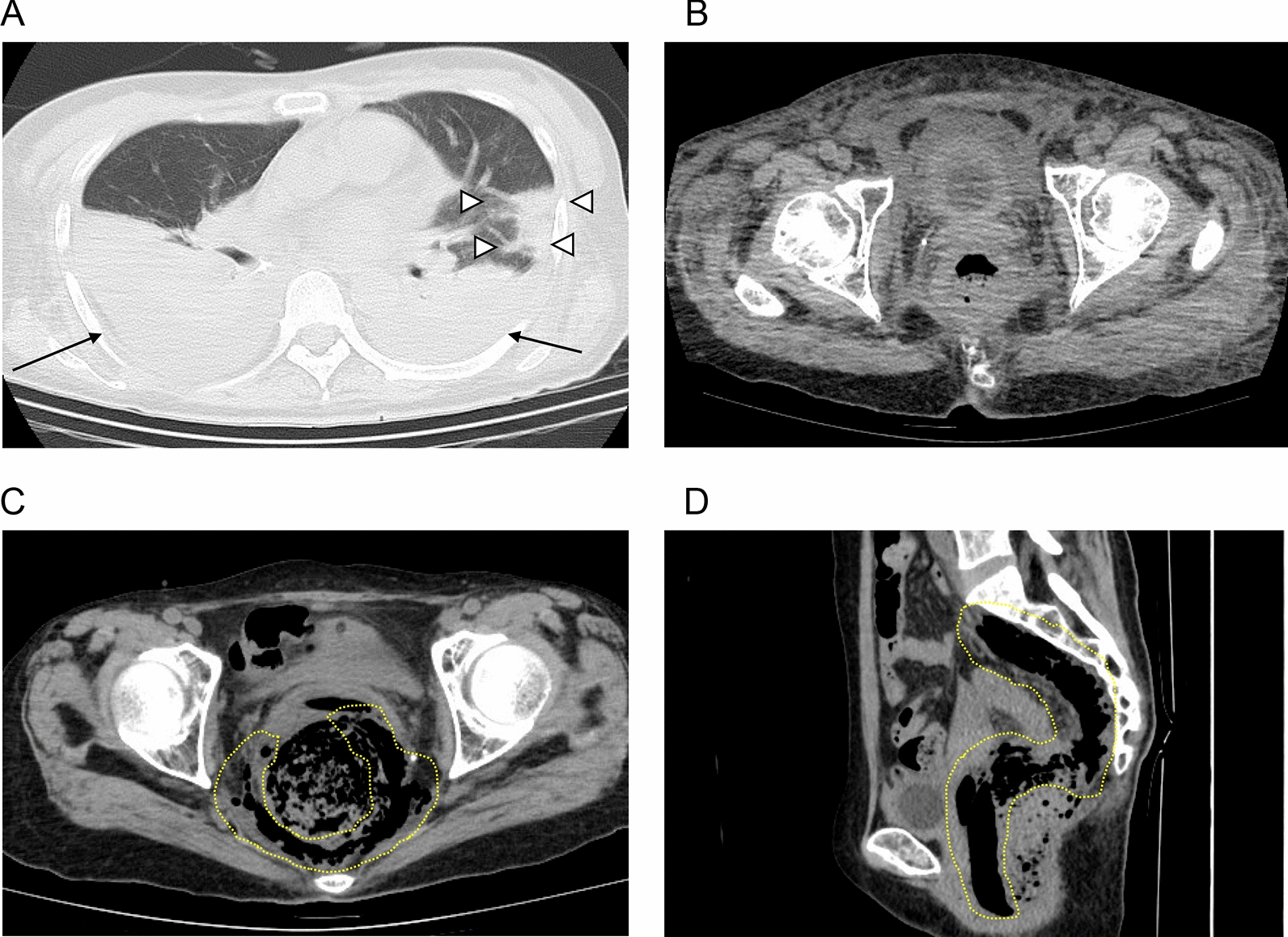
A contrast-enhanced computed tomography (CT) scan revealed slightly irregular pleural thickening from the base to dorsal pleura of the left lung and a more tangential mass-like structure at the base of the left lung. There was no abnomality in the hilum. There were no obvious rib fractures. Since multiple nodules were found in both breasts, a consultation with a breast surgeon was recommended (Fig. 1).
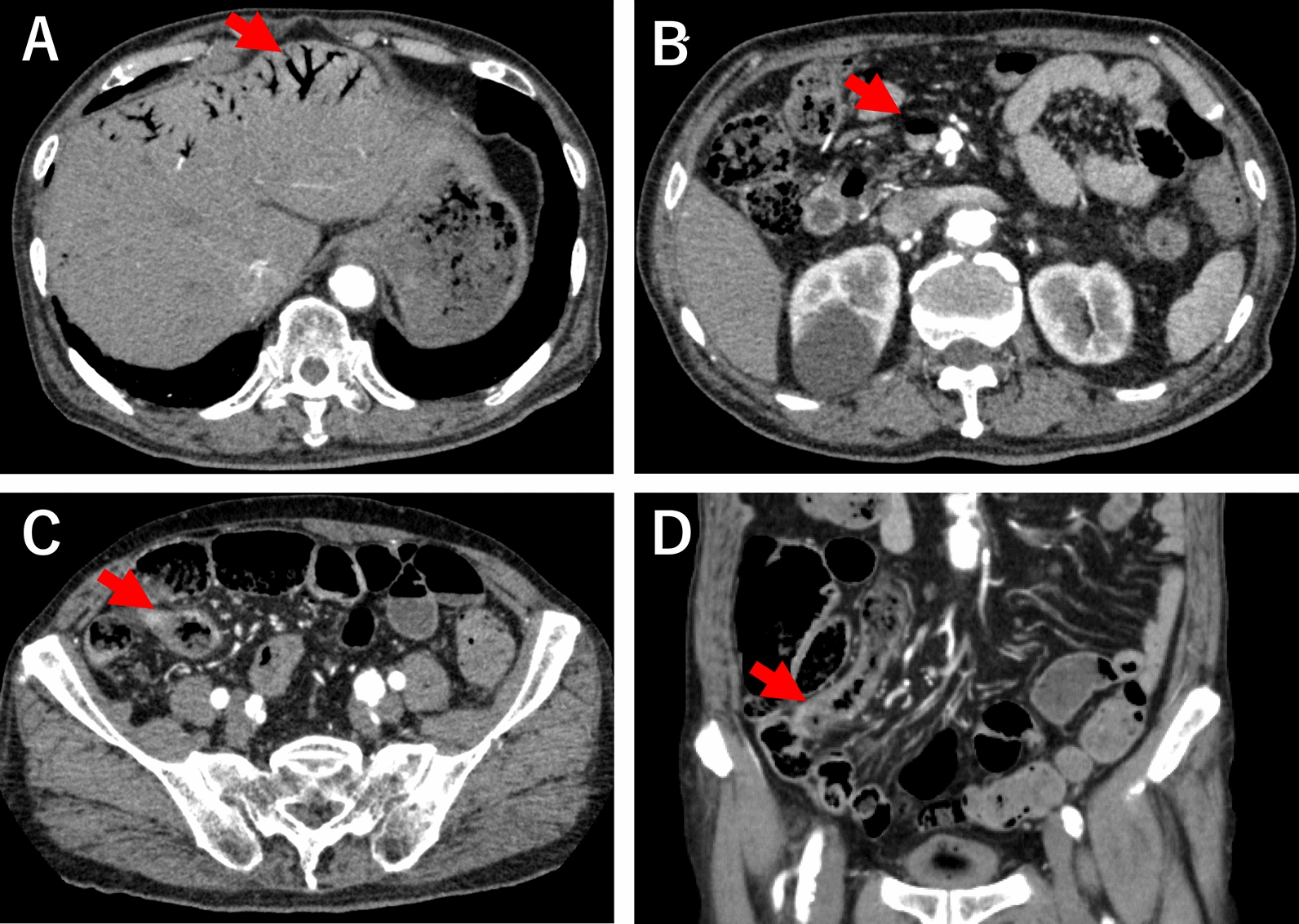
Fig. 1
A contrast-enhanced computed tomography (CT) scan revealed irregular pleural thickening and a more tangential mass-like structure at the base of the left lung. Multiple nodules were also revealed in both breasts
On palpation, an elastic, firm, well-defined, slightly poorly mobile mass of approximately 1–2 cm was palpated on the B resion of the right breast and the D resion of the left breast. No axillary or supraclavicular lymph nodes were observed.
Mammography revealed a round, well-defined, hyperintense mass in the left breast without calcification. The mass was not clearly visible in the right breast, but there was focal asymmetric density (Fig. 2).
Fig. 2
Mammography revealed a round, well-defined, hyperintense mass in the left breast. There was focal asymmetric density in the right breast
Ultrasonography showed multiple round, well-defined, full, hypoechoic masses with internal pulsatile blood flow signal. Elastography showed relatively uniform firmness. The multiple masses were showed in both breasts’ subcutaneous and mammary tissues. The largest masses were 7 mm in the B restion of the right breast and 6 mm in the D resion of the left breast, and the multiple masses were similar in shape. There were no bilateral axillary lymph node enlargements (Fig. 3).
Fig. 3
Ultrasonography revealed multiple round, well-defined, full, hypoechoic masses with internal pulsatile blood flow signal in both breasts. Elastography showed relatively uniform firmness
An ultrasound-guided needle biopsy was performed on the B resion of the right breast and the D resion of the left breast. Both breast masses were diagnosed as solid-type invasive ductal carcinoma of the breast. Furthermore, both had the same immunostaining characteristics of triple negative type, with negative estrogen receptor (ER), progesterone receptor (PgR), and human epidermal growth factor receptor2 (HER2) status. The pathology confirmed the diagnosis of triple negative primary bilateral multiple breast cancer (Fig. 4).
Fig. 4
Photomicrographs of the biopsied breast tumor sections. a–e are the right breast tissue, f–j are the left breast tissue. a, f Hematoxylin and eosin (H &E) -staining (magnification × 20), b, g (magnification × 40), c, h Immunohistochemistry of ER (magnification × 20), d, i PgR (magnification × 20), e, j HER2 (magnification × 20)
Contrast-enhanced MRI showed multiple masses with rim enhancement and hypo-diffusion in both breasts’ subcutaneous and mammary tissues. The largest masses were 13 mm in the B region of the right breast and 10 mm in the D region of the left breast, and all masses, including these masses, showed similar contrast patterns (Fig. 5).
Fig. 5
Contrast-enhanced MRI showed multiple masses with rim enhancement and hypo-diffusion in both breasts’ subcutaneous and mammary tissues
18F-fluorodeoxyglucose (FDG) positron emission tomography-CT showed a nodule with FDG accumulation (SUVmax = 11.42) in the left lower lobe. In addition, multiple other nodules were also found in the bilateral breasts, such as a 1.1 cm nodule (SUVmax = 6.27) in the left D region and a 1.1 cm nodule (SUVmax = 5.75) in the right B region in the breast subcutaneous tissue. Multiple FDG accumulations were also observed in the left pleura, diaphragm, supraclavicular fossa lymph node, and left parasternal lymph node. Notably, no significant FDG accumulations were observed in subcutaneous tissue other than the breasts (Fig. 6).
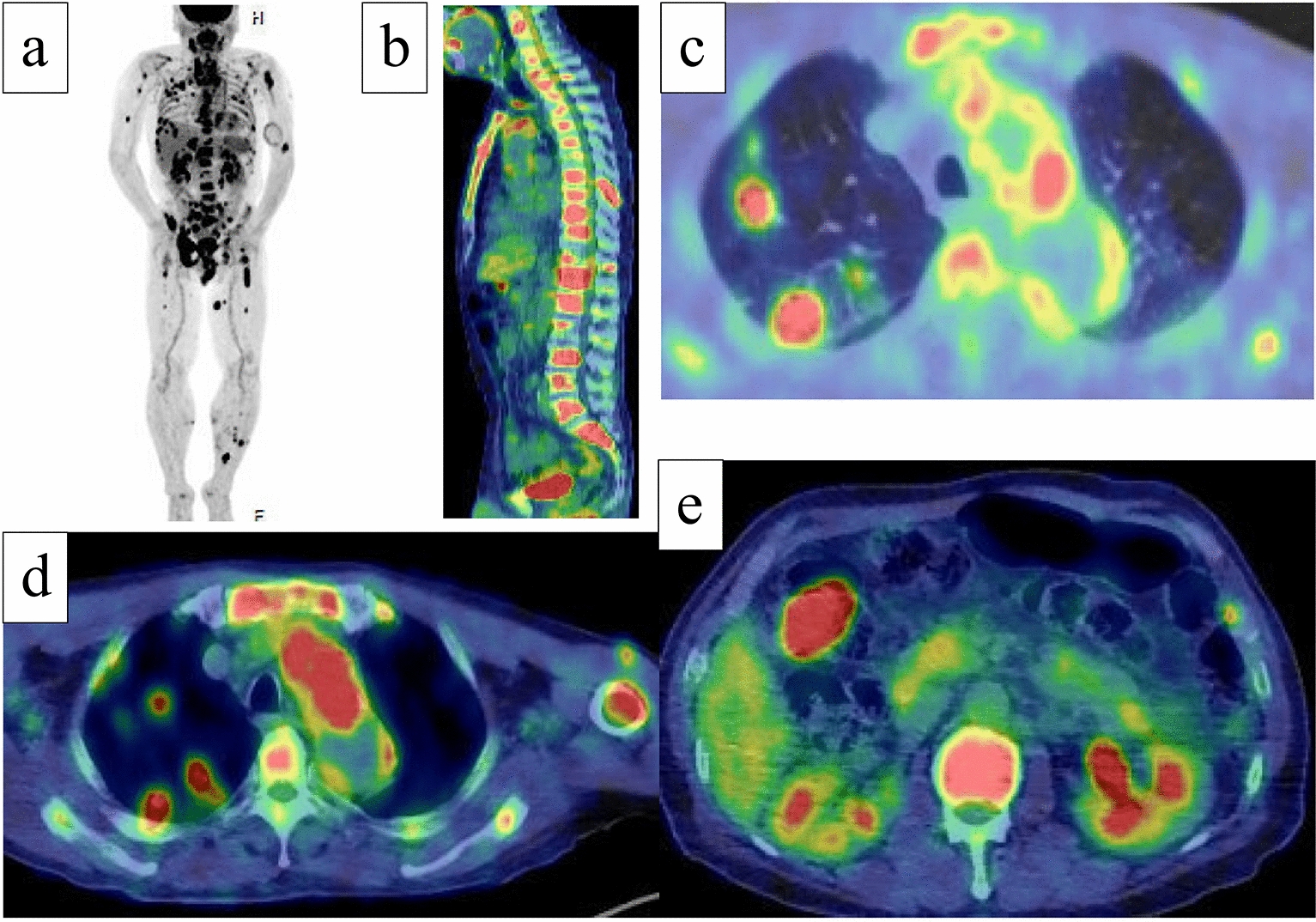
Fig. 6
18F-fluorodeoxyglucose (FDG) positron emission tomography-CT showed a nodule with FDG accumulation (SUVmax = 11.42) in the left lower lobe. Multiple FDG accumulations were also observed in the bilateral breasts
Blood tumor markers were high: progastrin-releasing peptide (ProGRP) 37,300 pg/ml (normal range, 0–81.0 pg/ml) and neuron-specific enolase (NSE) 35.0 ng/ml (normal range, 0–16.3 ng/ml). Carcinoembryonic antigen (CEA), carbohydrate antigen 15–3 (CA15-3), squamous cell carcinoma (SCC), sialyl Lewis X-i antigen (SLX), and cytokeratin fragment (CYFRA) were within the normal ranges.
Based on high ProGRP levels, we considered the possibility of primary lung cancer and performed a thoracoscopic biopsy. Pathological examination revealed atypical epithelial cells in a full or sporulated fashion, small cells with a high N/C ratio, and slightly larger cells with eosinophilic cytoplasm. ChromograninA ( +), synaptophysin ( +), CD56 ( +), thyroid transcription factor-1-TTF-1 ( +), and p40 (−) were the immunostaining characteristics of the cancer. Based on the above findings, the diagnosis of SNEC was made (Fig. 7).
Fig. 7
Photomicrographs of the biopsied lung lesion. a Hematoxylin and eosin (H &E) -staining (magnification × 20), b (magnification × 40), c Immunohistochemistry of ChromograninA (magnification × 20), d Synaptophysin (magnification × 20), e CD56 (magnification × 20), f thyroid transcription factor-1-TTF-1 (magnification × 20), g p40 (magnification × 20)
Additional immunostaining was performed on needle biopsies of bilateral breast masses (chromograninA ( +), synaptophysin ( +), CD56( +), thyroid transcription factor-1-TTF-1 ( +), cytokeratin AE1/AE3 ( +), LCA(−), E-cadherin ( +), napsin A (−), ER = 0%, PgR = 0%, HER2 = 0, Ki-67 = 30%). The immunostaining results of the bilateral breast masses were the same. Furthermore, the lung tissue from thoracoscopic biopsy also showed the same findings (Fig. 8).
Fig. 8
Photomicrographs of the biopsied breast tumor sections. a–d are the right breast tissue, e–h are the left breast tissue. a, e Immunohistochemistry of ChromograninA (magnification × 20), b, f Synaptophysin (magnification × 20), c, g CD56 (magnification × 20), d, h thyroid transcription factor-1-TTF-1 (magnification × 20)
The patient was finally diagnosed with bilateral breast metastases of primary SNEC. The patient was started on cisplatin, etoposide, and atezolizumab in the Department of Respiratory Medicine to treat stage IV small cell lung cancer.
留言 (0)