
記住我





A 76-year-old female with no past medical or family history presented to the hospital with the chief complaint of a right breast mass. During physical examination, two masses were palpated in the right breast. The first (No. 1) was a 56 mm right breast mass at the 10 o'clock position, while the second (No. 2) was a 21 mm large elastic hard mass at the 4 o’clock position. Imaging studies suggested the masses to be breast cancer as both showed compressible growth (Figs. 1, 2, 3). Core needle biopsy was performed on only the 5-cm-sized mass (No. 1) (Fig. 4). The results indicated an invasive breast carcinoma of no special type (NST) that was negative for ER, PR, and HER2. It was a poorly differentiated carcinoma with focal growth. Additionally, the other mass (No. 2) was clinically diagnosed as the same tumor as the first mass, but a needle biopsy was not performed.
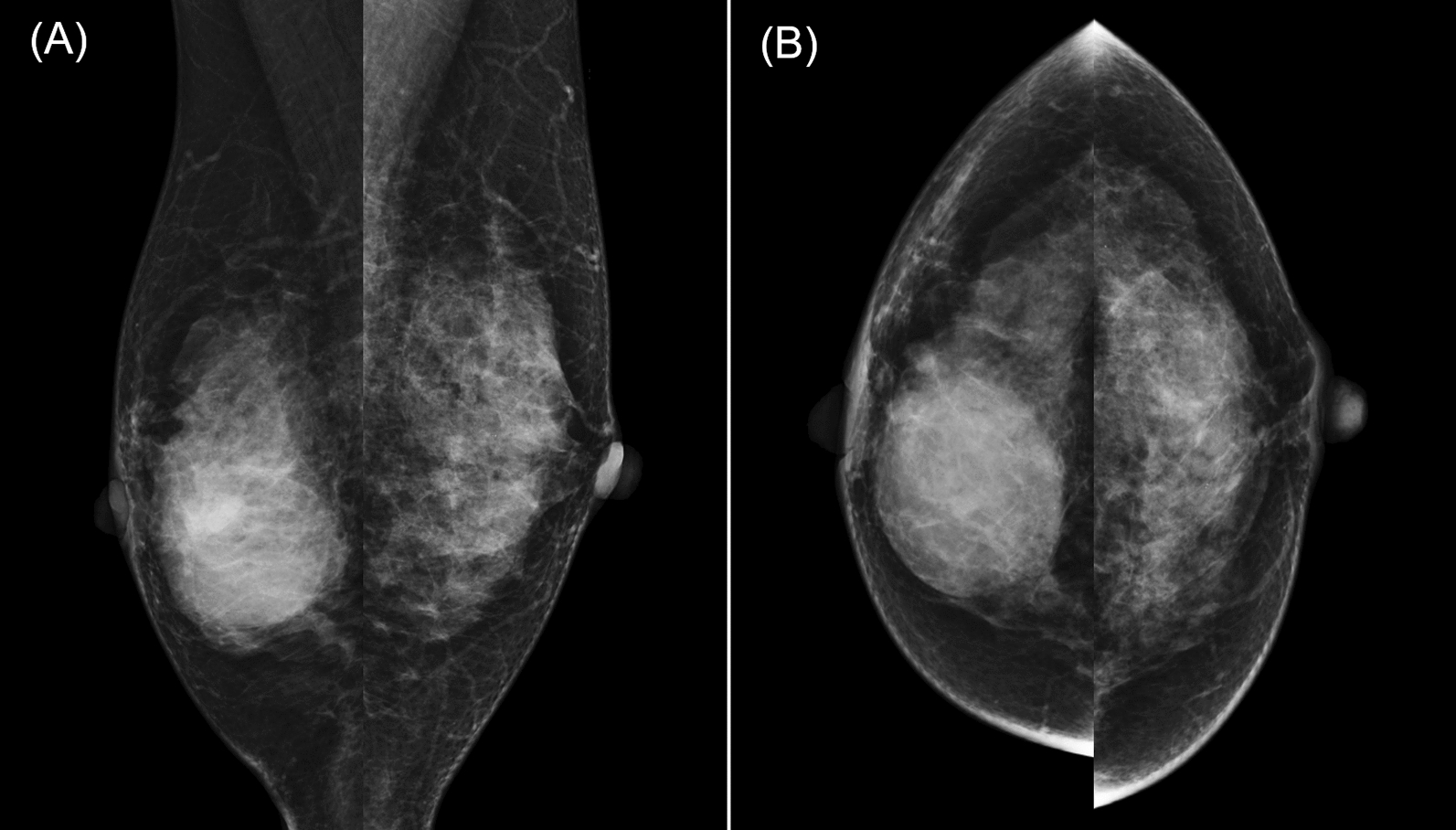
Fig. 1
Mammography. a, b displays the mediolateral oblique and craniocaudal views of the right breast mammography, respectively. Mass No. 1, indicated by a white arrow, is characterized as an oval, well-circumscribed, smooth-contoured, high-density lesion. In contrast, mass No. 2, marked by a yellow arrow, is depicted as an oval mass with an indistinct margin and high density. c displays an enlarged mediolateral oblique view
Fig. 2
Ultrasonography. a illustrates mass No. 1, characterized as a lobulated, well-defined, smooth-edged, hypoechoic lesion with a size of 56 mm located on the lateral aspect of the right breast. b depicts mass No. 2, which presents as an irregular, well-defined, and rough-edged hypoechoic lesion measuring 28 mm and situated on the medial aspect of the right breast
Fig. 3
Contrast-enhanced breast magnetic resonance imaging findings. a Mass No. 1 is depicted as a lobulated lesion with a somewhat irregular but distinct boundary, measuring 53 mm and located at the 9 o’clock position of the right breast. The lesion demonstrates a fast washout pattern on the time–intensity curve. Conversely, b illustrates mass No. 2 with a diameter of 26 mm situated in the inferomedial quadrant of the same breast. This mass is characterized by a border that is less well defined compared to mass No. 1 and exhibits a fast washout pattern on the time-intensity curve
Fig. 4
Hematoxylin and eosin-stained sections from core-needle biopsy of specimen No. 1. a–c depicts the neoplastic tissue at ×5, ×200, and ×400 magnifications, respectively. The diagnosis of mass No. 1 as invasive carcinoma is substantiated by the histopathological features of a poorly differentiated neoplasm exhibiting solid growth patterns with occasional alveolar structures. The tumor is assigned a nuclear grade of 3 and a histological grade of 3. Immunohistochemical staining results are negative for estrogen receptor and progesterone receptor, with a human epidermal growth factor 2 score of 0. The Ki-67 proliferation index is markedly elevated at 100%
The preoperative diagnosis was right breast cancer (T3N0M0 Stage IIB) of the TNBC subtype. The treatment team recommended preoperative chemotherapy, but the patient refused; therefore, surgical treatment (right breast mastectomy and sentinel lymph-node biopsy) was performed initially. The surgical and postoperative courses were uneventful, and the patient was discharged on postoperative day 8.
The histopathology results of the surgical specimen showed a malignant lymphoma with a tumor size of 38 × 17 mm, CD20 (+), CD45 (+), CD79a (+), CD3 (−), CD10 (−), and pancytokeratin (−), indicating diffuse large B-cell lymphoma (DLBCL). In contrast, the other tumor (No. 2) was an invasive breast carcinoma of NST, ER (+), PR (+), HER2 score: 0, pT2 (21 mm), and pN0 (sentinel lymph node). Pathologically, no continuity was found between the two tumors (Figs. 5, 6). We reassessed the core-needle biopsy specimen, noting that the tumor cells displayed a more lymphoid morphology than previously observed, which may be attributable to variabilities in tissue preparation, including potential artifacts introduced during needle biopsy and tissue fixation. Due to the diffuse proliferation of large lymphoid cells, immunostaining was conducted under the suspicion of malignant lymphoma. The tumor cells tested positive for CD20, CD45, CD79α, BCL2, and BCL6, and negative for CD3, CD5, CD10, cyclin D1, and cytokeratin AE1/AE3. These findings confirmed the diagnosis of diffuse large B-cell lymphoma (DLBCL) (Fig. 6).
Fig. 5
Pathological findings of surgical specimens No. 1 and No. 2. Fresh and formalin-fixed sections are shown in (a). Specimen No. 1 is described as a milky white, nodular mass, whereas specimen No. 2 is a milky white, lobulated mass; both are discrete without any interconnection. b–e displays escalating magnifications of Hematoxylin and Eosin staining, highlighting the homogeneous cell proliferation with a pronounced nucleus-to-cytoplasm ratio in specimen No. 1. Specimen No. 2 is typified by the classic hallmarks of invasive breast carcinoma of no special type featuring a solid growth pattern and nested infiltration
Fig. 6
Immunohistochemical profiling of surgical specimens No. 1 and No. 2 and core-needle specimens. a–c sequentially exhibit the immunoreactivity of mass No. 1 to CD20, CD10, and CD3 markers, each at ×200 magnification. d compares masses No. 1 and No. 2, demonstrating their staining patterns with cytokeratin AE1/AE3 at ×5 magnification. e, f exhibits the immunoreactivity of the core-needle biopsy specimen to CD20 and cytokeratin AE1/AE3 markers, respectively, each at ×100 magnification
Postoperative therapy consisted of endocrine therapy (letrozole) for breast cancer. For DLBCL, the patient was determined to be in Stage 1E after a systemic search and was treated with five courses of R-CHOP chemotherapy followed by three courses of intrathecal chemotherapy with methotrexate, cytarabine, and dexamethasone. At 2 years post-surgery, the patient was alive, and neither tumor had recurred.
留言 (0)