
記住我

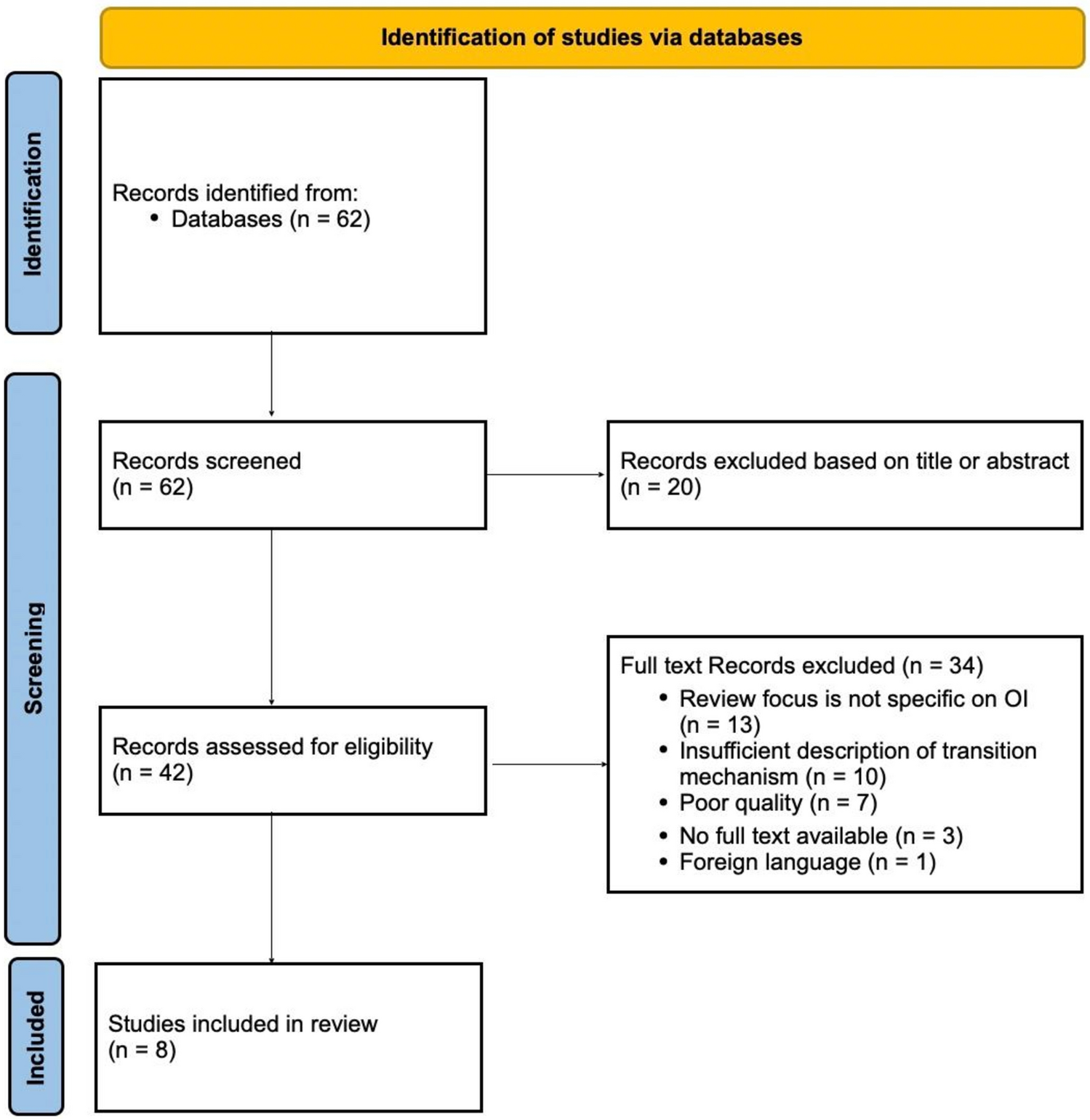







The literature search generated a total of 1195 references: 368 in Ovid/Medline, 497 in Embase.com, and 330 in Clarivate Analytics/Web of Science Core Collection. After removing duplicates of references that were selected from more than one database, 673 references remained. The flowchart of the search and selection process is presented in Fig. 2. Of the total 673 articles that were identified, 142 were included for full-text analysis. In total, 36 articles were included, all being large case series (n > 10), cohort studies, or case–control studies (Table 1) [3, 5, 10, 13,14,15,16, 18, 19, 25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. A quality assessment (Study Quality Assessment Tool by NHLBI [24]) of the included articles was performed by the two reviewers independently; 5.6% (n = 2) of the studies were classified as poor, 33.3% (n = 12) as fair; and 61.1% (n = 22) as good. Articles assessed as poor were excluded, resulting in 34 articles included in the qualitative synthesis.
Fig. 2
Flowchart of the search and selection procedure of studies
Table 1 Studies on dental abnormalities in osteogenesis imperfecta which are included in this reviewIncluded StudiesThis review includes case series, cohort studies, and case–control studies investigating dental issues in individuals with OI. Table 1 provides an overview of the selected studies, detailing aspects, such as the countries and inclusion periods, study designs (prospective or retrospective), the number of participants screened for dental abnormalities, demographic information including age ranges and gender distributions, clinical classifications of OI in the cohorts under study, and the abnormalities examined. Studies conducted on the same cohort were combined, with the results being discussed collectively as one study (Table 1): (a) Bendixen et al. [27], Gjørup et al. [29], Hald et al. [30], Thuesen et al. [15]; (b) Lindau et al. [32], Lindau et al. [33]; (c) Ma et al. [13], Taqi et al. [45]; Taqi et al. [46]; (d) Malmgren & Lindskog [37], Malmgren & Norngren [5]; and (e) Malmgren et al. [36], Andersson et al. [26]. Subsequent sections provide a summary of the literature pertaining to various dental problems reported in OI. The prevalence of DI and that of Class I, II, and III malocclusions in OI cohorts have been summarized in Tables 2 and 3, respectively.
Table 2 Prevalence of dentinogenesis imperfecta in the osteogenesis imperfecta cohorts included in this reviewTable 3 Prevalence of class I, II, and III occlusions in OI cohorts assessed using Angle’s classificationDental Abnormalities in Osteogenesis ImperfectaDentinogenesis Imperfecta and Related Dental FindingsStudies investigating DI in individuals with OI revealed a wide array of diagnostic approaches and criteria used to diagnose DI. For instance, while Majorana et al. and Sæves et al. considered discoloration alone as sufficient for diagnosis, Ma et al. required a combination of color change, attrition, and altered crown shape [13, 14, 35]. Although Sæves et al. diagnosed DI solely based on clinical observations of tooth color and translucency when visible signs were present, they used radiographic indicators, including tooth morphology anomalies, to diagnose DI in individuals without clinically visible signs [14]. Schwartz & Tsipouras and Thuesen et al. emphasize the necessity of multiple manifestations for diagnosis [15, 44], while many other studies do not state explicit diagnostic criteria. Table 2 categorizes these studies based on diagnostic methods: clinical, radiographic, histological, or a combination of these.
Four studies utilized histological evaluation to diagnose DI [25, 32, 33, 39]. Majorana et al. employed histology to confirm the diagnosis of DI [35], while others used it to analyze teeth from patients with and without DI based on clinical and/or radiographic assessments. Interestingly, histological examination performed by Andersson et al. identified nineteen additional cases of DI beyond those detected by clinical and radiographic methods (44/152 (29%) versus 63/152 (41%) [25]. Martìn-Vacas et al. discovered that while clinical signs of DI were evident in 41.2% of cases, and radiographic signs in 69.2%, morphological alterations were found in all teeth via scanning electron microscopy [39]. Similarly, Lindau et al. observed irregular tubules and obliterated pulps by histological examination in all OI types, irrespective of a DI diagnosis [33]. Malmgren & Lindskog did not diagnose DI histologically but set up a dysplastic dentine score (DDS) system to evaluate dysplastic manifestations in dentin, identifying a distinct cut-off value (DDS = 23) distinguishing healthy teeth from those of OI individuals with DI [37]. Interestingly, 8/17 (47%) of OI individuals without clinical signs of DI exhibited a DDS within the range observed in OI individuals with DI. All other studies relied on clinical and radiographic assessment for DI diagnosis, except for two that solely used radiographic evaluation (Table 2) [31, 38].
The prevalence of DI exhibited significant variation, both overall and within different OI types (Table 2). Among the four studies involving over 100 participants, employing clinical and/or radiographic evaluations in the same center, the overall prevalence ranged from 20 to 48% [13, 16, 25, 34]. Specifically, the prevalence within OI type I, III, and IV ranged from 9.8 to 31%, 56 to 86%, and 36 to 71%, respectively. Notably, while Andersson et al. and Malmgren et al. focused solely on dental abnormalities in children [16, 25], Ma et al.’s study encompassed both children and adults, with participants spanning up to 75.8 years of age [13]. Maioli et al. also included both children and adults [34]. In line with the aforementioned studies, with the exception of the study by Elfituri et al. [3], OI type I demonstrated the lowest prevalence of DI across all studies, consistently showing a prevalence more than two times lower than that of individuals with OI type III or IV [34]. Among eighteen studies reporting DI prevalence for both OI type III and OI type IV individuals, DI prevalence was found to be higher in OI type III individuals compared to those with OI type IV in eleven studies (Table 2). Two studies, by Kim et al. and Retrouvey et al., focused on individuals with OI type V, conducting both clinical and radiographic assessments [31, 42]. None of these individuals showed signs of DI. Mohd Nawawi et al. also included an individual with molecularly confirmed OI type V who did not have DI [40]. In contrast, a single case of DI in an OI type V individual (without genetic confirmation) was reported in a Japanese nationwide survey [41].
In the study by Andersson et al., 122/152 (80%) of OI patients had a COL1A1 or COL1A2 variant known to affect the formation of the collagen type I protein. Among those with predicted structurally abnormal collagen, 46 (70%) were diagnosed with DI, whereas only 15 (27%) with a quantitative defect had DI. In patients without an identified variant in COL1A1 or COL1A2, 6.9% had DI [25]. Thuesen et al. found DI in eighteen individuals, of whom 94% had a qualitative collagen defect, whereas 5.6% had a quantitative defect [15]. Maioli et al. found that 43/58 individuals with DI (74.1%) exhibited a variant in either COL1A1 or COL1A2. They observed that qualitative defects were more commonly associated with the occurrence of DI compared to quantitative defects (35.6% versus 16.7%). Among patients with glycine substitutions, 21/59 (35.6%) developed DI; yet, none had DI when the substitution occurred within the first 127 amino acids of the COL1A1 helical domain. Yamaguti et al. additionally distinguished between the two collagen type I genes. In their cohort of 81 individuals, they found that 84% of patients with a defect in COL1A2 had DI, whereas only 36% with a defect in COL1A1 exhibited DI [48]. These findings align with results from other studies. As the authors noted, defects in COL1A1 were more likely to result in quantitative collagen type I defects, while defects in COL1A2 were more likely to lead to qualitative defects. Taqi et al. did not directly address DI but noted that in their OI cohort (n = 154) tooth discoloration was more prevalent in individuals with certain COL1A1 and COL1A2 variants, particularly those with helical glycine substitutions (39% and 37%, respectively), compared to splice site variants (18%) or COL1A1 haploinsufficiency (4%). COL1A1 haploinsufficiency showed the lowest prevalence of pulp obliteration, a clinical sign of DI [45].
DI prevalence tended to be higher in deciduous teeth compared to permanent ones. O’Connell & Marini found that 82% and 83% of deciduous teeth in OI types III and IV patients, respectively, showed discoloration, while only 36% and 65% of permanent teeth were affected. Attrition and enamel fractures were more pronounced in yellow–brown-discolored deciduous teeth [10]. Nguyen et al. also reported higher DI rates in deciduous teeth (52%) compared to permanent dentition (44%) [18]. Andersson et al. investigated both deciduous and permanent dentitions of 40 individuals with DI; half of these showed DI symptoms in both sets of teeth, while the other half only had DI in deciduous dentition. This led them to hypothesize that individuals without DI in permanent teeth may have had DI in their deciduous dentition. No individuals showed DI signs solely in permanent teeth without any in deciduous teeth [25]. Lindau et al. observed that 71% of individuals with deciduous teeth exhibited DI, while only 50% of those with permanent teeth had the condition [33]. Maioli et al. did not specify the dentition type, but they categorized their cohort based on age. They identified DI in 18/167 adults (10.8%) and 40/174 children (23.0%) [34].
In a case–control study by Vuorimies et al., the prevalence of DI was compared between children with OI who received bisphosphonates (BP) treatment and those who did not. They found abnormal dentin in 23% (5/22) of the BP-treated group and 38% (19/50) of the untreated group. The BP-treated group had a slightly higher proportion of OI type I subjects compared to the untreated group (73% versus 66%) [47]. Similarly, Malmgren et al. conducted a case–control study assessing DI prevalence among children with OI, categorized by BP treatment and age at treatment initiation. The overall prevalence of DI was 20% (44/219), with a combined prevalence of 33% (18/55) among BP-treated groups and 16% (26/164) among the untreated group. Despite these differences, statistical analysis did not show significant disparities between the groups. Notably, OI type I predominated in the untreated group (80%), whereas in the BP-treated groups, it averaged around 40% [
留言 (0)