Pituitary hormones play a crucial role in regulating skeletal physiology, and bone fragility is a frequent consequence of pituitary disorders [1]. The clinical relevance of pituitary hormone actions on bone metabolism is demonstrated by the often-severe skeletal damage seen in conditions of hyperfunction or hypofunction of the gland [1].
In the general context of osteoporosis, fragility fractures represent the most important clinical outcome, as they directly reflect the severity of bone damage and are linked to increased disability, morbidity and mortality [2, 3]. Therefore, essentially all clinical actions that are put in place in this area have the ultimate aim to predict fracture risk and, consequently, to implement timely therapeutic actions able to reduce the probability of fracture events in primary or secondary prevention [2, 3].
In the setting of primary osteoporosis, several factors have been identified as predictors of an individual’s fracture risk [4, 5]. Over the years, these factors have also been combined into various integrated predictive tools, that have been developed and extensively validated for fracture risk prediction [6,7,8]. Among these, the one that is most widely used is FRAX®, which combines several clinical risk factors with bone mineral density (BMD) to calculate the 10-year probability of hip fracture and the 10-year probability of a major osteoporotic fracture (clinical spine, forearm, hip or shoulder fracture) [6].
In the setting of secondary osteoporosis, obtaining a reliable estimate of fracture risk can be much less straightforward [1, 9]. Some fracture risk calculators, including FRAX® itself, provide the possibility of reporting the presence of a condition causing secondary osteoporosis [6]; however, this is included in the calculator as a non-specific information, without the ability to differentiate between different causes of secondary osteoporosis, nor to further stratify the assessment of fracture risk according to any additional parameter, such as disease duration and/or severity.
Moreover, the reliability of these risk calculators has been much less extensively validated in the contexts of secondary osteoporosis, and their generalizability is not obvious, given the different pathophysiology of bone damage in each disease [1, 9]. The classic predictors used in FRAX® are in fact often much less informative in the context of secondary osteoporosis [1, 9]. The clearest example of this is probably represented by the role of BMD: indeed, while accounting for more than two-thirds of the whole bone strength in primary osteoporosis, in the contexts of secondary osteoporosis its measurement is much less informative about fracture risk, if at all [1, 9]. In fact, bone fragility in secondary osteoporosis is much more significantly influenced by alterations in bone quality and microarchitecture, which are not captured by BMD [1, 9, 10].
In recent years, many efforts have been made to overcome this limitation by introducing techniques capable to noninvasively assess bone quality, such as trabecular bone score (TBS) [10,11,12] and high-resolution peripheral quantitative computed tomography (HR-pQCT) [13, 14], among others. These parameters have been evaluated in several forms of secondary osteoporosis [15,16,17,18,19,20,21], often with promising results. However, given the relative rarity of these conditions, the sample sizes of these studies cannot match those available for primary osteoporosis, and the lack of adequate follow-up is often a significant limitation. Additionally, bone turnover markers have emerged as well as important tools in evaluating bone metabolism and turnover, providing further insights into fracture risk assessment [22, 23].
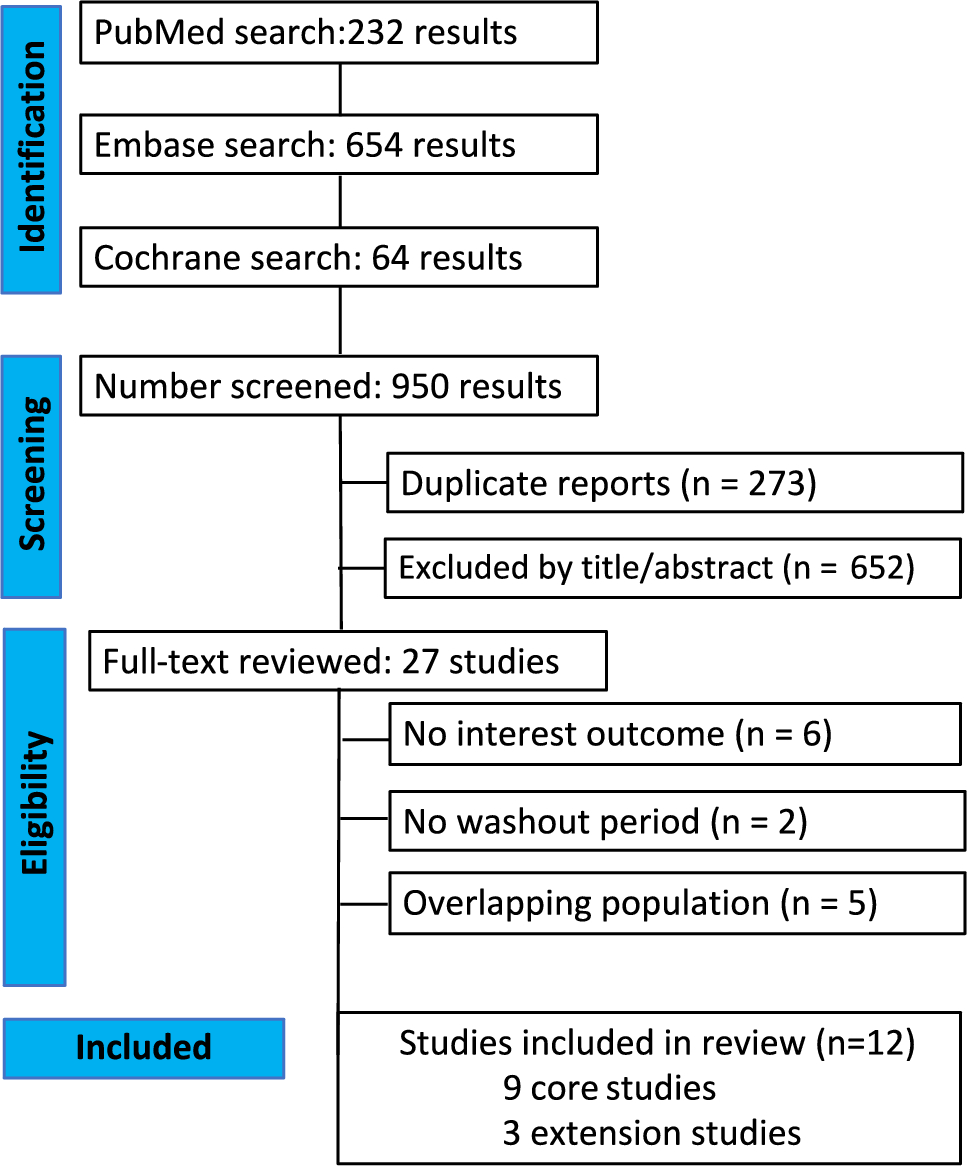
The aim of this review is to address the clinical question of fracture risk prediction in patients with pituitary disease, evaluating the available evidence about predictors of fragility fractures in each context of hyperfunction or hypofunction of the gland.
Acromegaly
Traditionally, growth hormone (GH) and insulin-like growth factor 1 (IGF-1) were viewed as anabolic hormones that benefit the skeleton by promoting longitudinal bone growth, bone modeling, and remodeling [24]. However, in the last two decades, compelling evidence showed that a pathological GH excess actually contributes to skeletal fragility, sustained by increased bone turnover and abnormalities in bone microstructure, ultimately raising fracture risk [25,26,27]. Fractures are frequently asymptomatic and predominantly involve the thoracic spine, with anterior wedge deformities leading to kyphosis [28].
The risk of fractures is tightly related to the exposure to elevated GH and IGF-1 levels. The prevalence of vertebral fractures at diagnosis has been shown to be correlated with a longer estimated diagnostic delay [29] and with higher random serum GH levels [30]. Moreover, during the course of the disease, patients with active acromegaly are characterized by a markedly higher fracture risk compared to those with a biochemically controlled disease [27, 31]. Of note, an effect related specifically to the individual drugs used for the medical treatment of acromegaly may also be present, with some evidence supporting a lower fracture risk in patients with biochemically active disease treated with pasireotide compared to those treated with pegvisomant [32].
Acromegaly is not characterized by a significant alteration of BMD [26], with most patients showing normal or even increased bone density at various skeletal sites, in large part due to different distribution of trabecular and cortical bones, concomitant joint degenerative disorders characterized by osteophytes and facet joint hypertrophy, increased periosteal ossification and bone enlargement [1]. In line with these findings, BMD does not represent a reliable predictor of fractures in the setting of acromegaly; in fact, studies comparing acromegalic patients with and without VFs did not find any significant difference in BMD between the two groups, and VFs occurred even in patients with normal bone density [26, 33].
Currently, new tools are being studied to assess bone quality and predict fracture risk in acromegalic patients. The TBS, for example, has been found to be lower in acromegalic patients than in non-acromegalic controls, and was significantly lower in acromegalic patients with prevalent VFs than in those without [15]. Similar data of impaired bone quality can be captured by HR-pQCT, with studies showing an alteration of both cortical and trabecular microarchitectural parameters [34, 35]. Bone microindentation, a micro-invasive method that measures bone material strength by a probe on the tibial surface, showed lower values in acromegaly patients even after biochemical control, thus suggesting persistence – at least to a certain degree, of cortical bone alterations [36]. Other indices and techniques, such as quantitative ultrasound (QUS) and 3D-SHAPER, have also been investigated as measures of skeletal health in acromegalic patients [37,38,39]. Overall, however, up to date there is no clear longitudinal data demonstrating a role of these indices as reliable predictors of incident fractures in this setting.
As in primary osteoporosis, a strong relationship between prevalent and incident VFs has been demonstrated also in acromegalic patients [40, 41]. In light of this, morphometric assessment of VFs even in the absence of specific symptoms and signs has to be considered as the cornerstone in the assessment of skeletal fragility in all patients with acromegaly, with an initial evaluation at diagnosis and subsequent regular monitoring during follow-up [30, 42], at intervals tailored to each subject’s evolving clinical condition, with special attention to male patients, patients with untreated hypogonadism, history of non-traumatic VFs, decrease in BMD, kyphosis, and biochemically active disease [26, 30, 41]. Of note, similar again to primary osteoporosis, fracture risk is also negatively associated with vitamin 25(OH)D levels, and appears to be reduced by cholecalciferol supplementation [43].
In terms of bone turnover markers, conventional and novel markers such as serum osteocalcin, bone-specific alkaline phosphatase (BALP), C-terminal telopeptide of type I collagen (CTX), procollagen type 1 N-terminal propeptide (P1NP) and sclerostin have been investigated to assess bone turnover in acromegaly [33, 44,45,46]. Elevated levels of these markers may correlate with an increased skeletal fragility and may serve as additional tools for evaluating bone health in these patients, although their exact role in predicting fracture risk requires further longitudinal studies.
Cushing’s disease
Endogenous hypercortisolism is an established cause of osteoporosis and bone damage, with fragility fractures representing in some cases the presenting clinical feature of the disease [47, 48]. From a pathophysiological point of view, glucocorticoid-induced osteoporosis is determined mainly by decreased bone formation, and to some extent by a slight initial increase in bone resorption, with a greater impact on trabecular compared to cortical bone [49].
Literature data indicate that fractures caused by glucocorticoid excess may represent an early event during the course of the disease [50,51,52], but their occurrence then increases with the duration of hypercortisolism [53]. The risk of fractures is also related to the severity of glucocorticoid excess, with a direct correlation with 24 h urinary free cortisol even after adjustment for multiple confounders [53, 54]. Interestingly, vertebral and rib fractures were significantly more common in men than in women in some research, but this difference could possibly be related to sex-specific differences in disease activity [54, 55]. Of note, fracture risk significantly decreases after adequate cure or treatment, together with an improvement in bone mineralization [51, 56, 57].
Differently from acromegaly, the measurement of BMD by DXA retains an independent prognostic role for the prediction of fracture risk in patients with endogenous hypercortisolism [55, 58, 59]. A decrease in BMD was consistently reported in patients with Cushing’s syndrome, with an increase in the prevalence of osteopenia and osteoporosis compared to controls [53, 60]; more specifically, in agreement with the notion that trabecular bone is more impacted by glucocorticoids than cortical bone, lumbar spine BMD tends to be impacted more than the hip and the forearm [49]. Moreover, several studies demonstrated a correlation between BMD reduction and fracture risk, with BMD values being a significant predictor of fractures both in treated and in untreated patients [55, 58,59,60].
Notably, however, the detrimental effects of glucocorticoid excess on bone health are not limited to a loss of bone mass [47, 48]. Patients with Cushing’s syndrome may often present fragility fractures even with mild or no reduction in BMD, and the increase in fracture risk overall exceeds the one that could be expected based on the reduction of BMD alone [53,54,55, 59]. In recent years, therefore, several studies have tried to fill this gap by evaluating indices of bone quality. TBS has been shown to be significantly lower in patients with Cushing’s syndrome than in controls [61], and lower TBS values have been generally reported in Cushing’s disease patients with prevalent VFs than in those without [20, 42, 61,






留言 (0)