
記住我






A comprehensive search encompassing PubMed, Medline, and Google Scholar was conducted, utilizing various combinations of keywords such as ‘humeral classification’ along with ‘bone loss,’ ‘defect,’ ‘revision,’ and ‘shoulder arthroplasty.’ All peer-reviewed journals were surveyed, and articles detailing classification systems for PHBL associated with rTSA were analyzed. Additional cross-referencing of the selected articles was conducted to identify further relevant literature for the study. Furthermore, the authors proposed a new classification, which underwent evaluation for inter- and intra-observer reliability utilizing weighted kappa coefficients as assessed by two independent orthopedic surgeons. The level of agreement was interpreted according to the Landis and Koch [6] criteria, where a score exceeding 0.80 denotes excellent agreement, 0.61–0.80 indicates good agreement, 0.41–0.60 signifies moderate agreement, 0.21–0.40 suggests fair agreement, and 0.20 or lower indicates poor agreement.
The McLendon et al. classificationIn 2017, McLendon et al. [7] introduced surgical indications based on whether bone loss was measured as being less than or exceeded 5 cm from the top of the medial humeral tray to the medial humeral shaft. The authors suggest considering an allograft prosthesis composite (APC) [8] once this 5-cm threshold is surpassed. This indication, initially developed to predict the need for a larger diaphyseal allograft affecting the deltoid insertion, was later expanded by Cox and McLendon [9] to cover all bone loss types in revision surgery (Fig. 1). It categorizes PHBL into several types: type I, less than 5 cm of bone loss, typically no allograft needed; type IB, asymmetrical loss, less than 5 cm medially, more laterally; type IC, intact cement mantle that needs revision for rotational stability; type II, 5–10 cm of loss, shorter allografts recommended; type III, over 10 cm of loss with a compromised deltoid. Humeral stem diameter and the cement-within-cement technique were also assessed for failure rates.
Fig. 1
This classification is an upgrade of McLenon et al. classification
Boileau’s classificationIn 2018, Boileau [10] suggested a classification system based on three types of PHBL: type A, with < 2 cm of epiphyseal bone loss; type B, with < 4 cm of metaphyseal bone loss; and type C, with > 4 cm of bone loss extending into the diaphysis. Introducing this stratification, he recommended using a 4-cm threshold to distinguish between cementoplasty reconstruction and APC, while minor humeral shortening can be addressed by adjusting the glenosphere, liner, or humeral tray. In 2020, Boileau [11] provided a modification of the previously described classification, basically changing type C to > 4 cm of bone loss extending into the diaphysis but < 8 cm of bone loss (above the “V” deltoid insertion) and adding type D, which corresponds to > 8 cm of bone deficit (below the V deltoid insertion). This modification was necessary as all cases analyzed exhibited more than 4 cm of PHBL, necessitating the subdivision of the cohort into two distinct subgroups (Fig. 2). This classification system has long served as a valuable reference for shoulder surgeons preparing for rTSA. However, these indications rely on specific absolute values that may not universally apply to all patients due to anatomical size variations.
Fig. 2
Schematic representation of the Boileau classification.
The PHAROS classificationIn 2018, a consensus group introduced the PHAROS classification [12]. This classification emerged from a comparative retrospective radiographic case series evaluation, aiming to anticipate the complexity of humeral reconstruction.
The objectives of this study were to establish a classification system for PHBL in rTSA based on plain radiographs alone and to provide therapeutic information to the surgeon. In the context of rTSA, this classification system can assist surgeons in making crucial clinical decisions, including the choice of using allograft, a higher liner, and/or higher polyethylene, cementoplasty, or massive tumoral prosthesis.
PHAROS type 1 describes epiphyseal bone loss encompassing the articular surface, tuberosities, and calcar. The classification further distinguishes between type 1C, indicating calcar loss, and type 1G, indicating loss or malunion of the greater tuberosity. Type 1 constitutes approximately 31% of all rTSA cases. PHAROS type 2 describes metadiaphyseal bone loss situated proximal to the deltoid attachment. Subtype 2A denotes cortical thinning of the metadiaphysis exceeding 50% of the expected cortical thickness, while subtype 2B involves the loss of both metadiaphyseal bone proximal to the deltoid and epiphyseal bone. PHAROS type 3 describes diaphyseal bone loss extending below the deltoid attachment. Subtype 3A indicates cortical thinning of the diaphysis exceeding 50% of the expected cortical thickness, while subtype 3B means that most of the diaphysis is compromised and there is epiphyseal and metadiaphyseal bone loss (Fig. 3).
Fig. 3
Schematic representation of the PHAROS classification
The PHAROS classification system acts as an algorithm that provides a framework for surgical planning. For type 1C and type 1G defects, stem fixation through cement augmentation alone may be a valid option, leaving the stem proportionately elevated to restore height. Special attention is required for type 1G defects to restore anatomical tuberosity positioning and ensure excellent fixation. Type 2A defects may necessitate the consideration of a proximal humeral allograft, depending on the quality and nature of the native bone encountered intraoperatively. More definitive plans should be made for type 2B defects, likely involving the use of a proximal humeral allograft. Type 3A defects might require a long proximal humeral allograft or a femoral allograft, which can extend through the metadiaphysis. Type 3B bone defects are ideally treated with massive tumoral prosthesis.
The PHBL-SCOReThe Proximal Humeral Bone Loss—Specific Classification for Optimal Reconstruction (PHBL-SCORe) is a novel diagnostic and therapeutic algorithm proposed by the authors. This classification system was designed to categorize proximal humeral bone loss in a clear, easily reproducible, and tailored method, with the aim of suggesting the most suitable treatment approach for each patient.
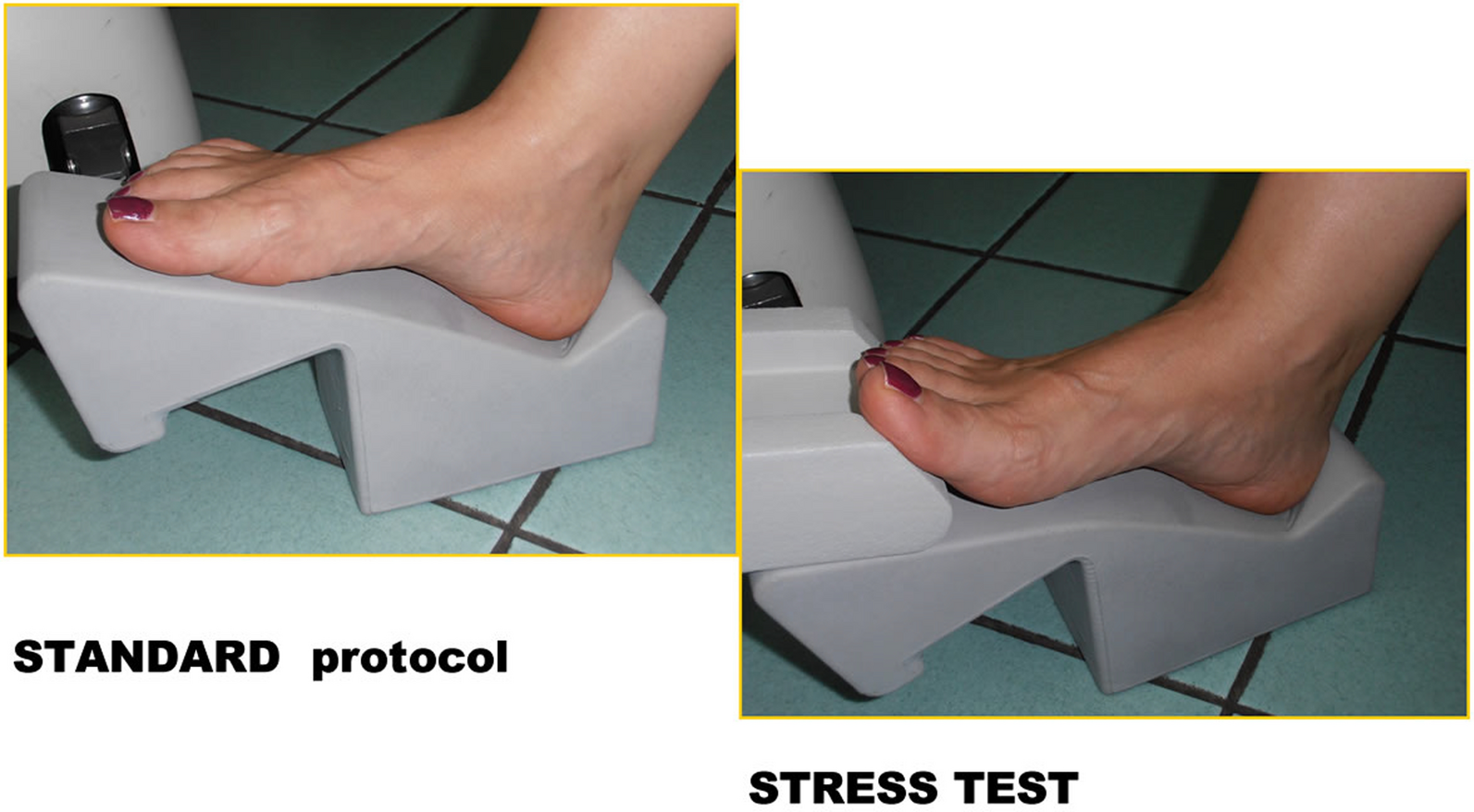
For the preoperative planning protocol, patients underwent an AP radiograph of the entire humerus, including both the limb scheduled for surgery and the unaffected limb. Radiographs were uniformly obtained at the same center, and all the radiographs were conducted following the same standardized radiographic protocol described by Lädermann et al. [13].
Radiographic measurements were obtained from scaled bilateral preoperative true antero-posterior images of the humerus. Those images were taken with patients standing and their shoulders in neutral rotation. Careful alignment of the humeri against the cassette ensured optimal image capture, with the X-ray beam focused on the middle third of the humerus. To account for magnification, a marker of known diameter was placed adjacent to the lateral humerus on the skin. Three primary lines were marked on the films for measurement in the healthy humerus and served as the “reference unit:” the trans-epicondylar line (line y), the diaphyseal axis (axis t), and a line that was perpendicular to the diaphyseal axis and passed through the highest point of the greater tuberosity. The segment of axis t between these perpendiculars was measured as m.
Three other three primary lines were marked on the film for measurement in the affected humerus: the trans-epicondylar line (y2), the diaphyseal axis (axis t2), and a line that was perpendicular to the diaphyseal axis and passed through the most prominent point of the residual proximal cortex. The segment of axis t2 between these perpendiculars was measured as m2.
The recorded values of m and m2 were used to extrapolate the predicted percentage of bone loss using the following formula: %bone loss = (m2/m) × 100 (Figs. 4, 5).
Fig. 4
Schematic representation of the measurement of proximal humeral bone loss expressed as a percentage
Fig. 5
True anteroposterior bilateral scaled radiographs of humeri, captured with neutral rotation and the patient in a standing position. The humeri were laid flat against the cassette, and the X-ray beam was precisely directed at the middle third. To account for magnification, a centimeter marker was strategically positioned laterally to the humerus
Two authors independently examined all the radiographs in a blinded manner using the Horos® viewer. Measurements were individually collected by each author following the established protocols. Subsequently, the gathered data were grouped together and compared to assess their reproducibility.
The inter-reliability evaluation between the two orthopedic surgeons expressed as the kappa coefficient was 0.798.
Based on this preoperative algorithm, our recommendation for classification and surgical treatment is the following:
Type A::Proximal humeral bone loss < 5%; treatment: increase in size of the metal liner and/or polyethylene
Type B::Proximal humeral bone loss > 5% and < 15%; treatment: increase in size of the metal liner and polyethylene + cementoplasty
Type C::Proximal humeral bone loss > 15% and < 40%; treatment: APC/minimal tumoral prosthesis
Type D::Proximal humeral bone loss > 40%; treatment: massive tumoral prosthesis.
Reconstruction optionsRevision reverse shoulder arthroplasty without allograftIn cases where bone defects are confined to the epiphysis, opting for a cemented revision without employing an allograft is a viable approach. The adequacy of the length can be assessed intraoperatively by using a trial component before cementation, considering factors such as soft-tissue and axillary-nerve tension, the force needed for inferior subluxation of the humerus, and the force required for prosthetic dislocation. Various methods can be employed to restore humeral length. One straightforward technique involves cementing the humeral stem in a proud position determined during preoperative planning and trialing. However, depending on the implant system, there are alternative approaches to modify the functional length of the humerus, such as metal augmentation at the stem–bone interface or utilizing a thicker polyethylene tray. Additionally, adjusting the size of the glenosphere or using an inferiorly eccentric glenosphere can influence joint stability and soft-tissue tension, compensating for minor deficits in humeral length. In some instances, a cementoplasty reconstruction may be necessary, involving the creation of a cement collar around the implant to restore the correct wrapping of the deltoid muscle (Fig. 6).
Fig. 6
Cementoplasty reconstruction
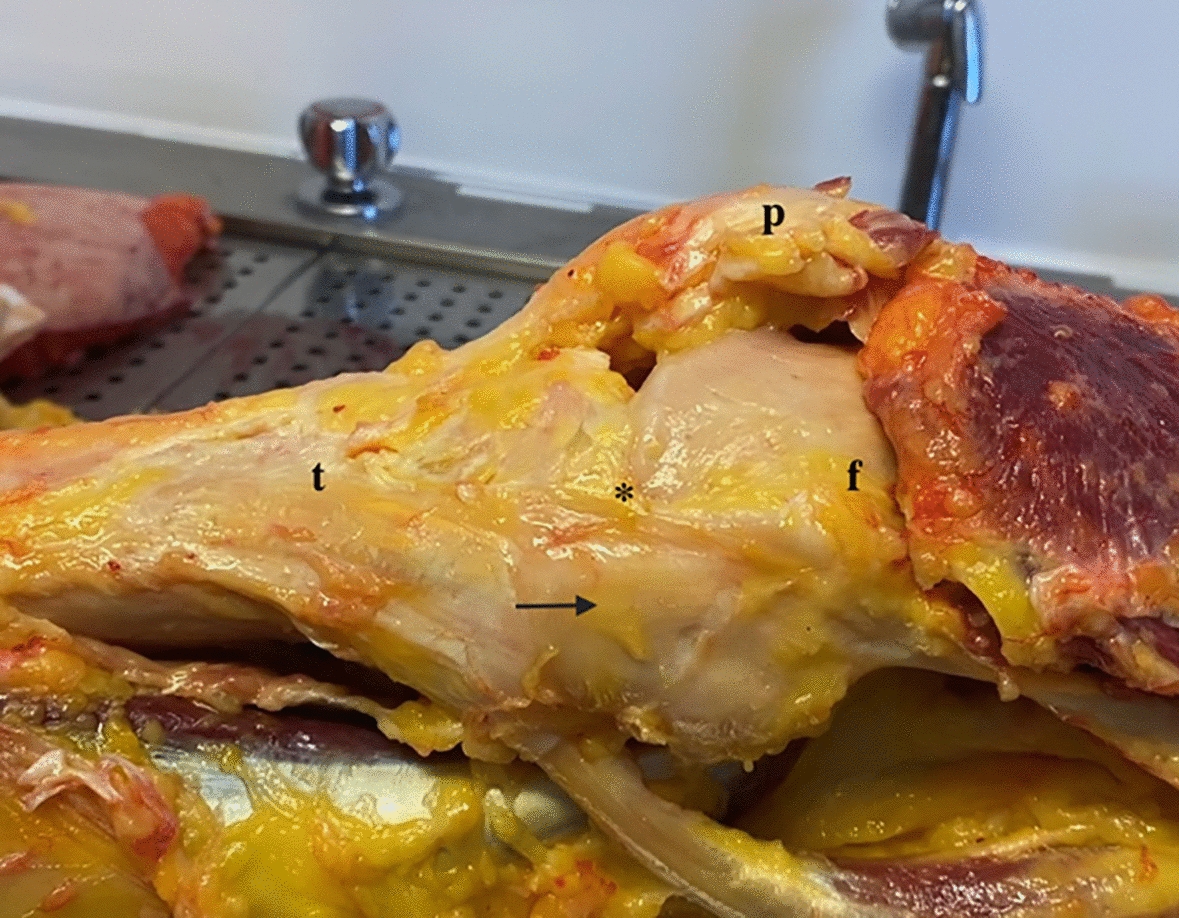
Allograft prosthesis composite using a proximal humeral allograftIn cases where bone defects extend into the meta-diaphysis, employing a proximal humeral allograft proves to be an excellent method to address bone loss and provide structural reinforcement to the humeral stem. The advantages of utilizing a proximal humeral allograft include enhanced structural support for the component, restoration of the humeral length and lateral offset, regeneration of bone stock, and attachment sites for soft-tissue structures such as the posterior cuff, subscapularis, and deltoid. Moreover, in the context of rTSA, the increased lateral offset offered by the allograft may positively impact the wrapping of the deltoid muscle. Following the removal of the previous humeral stem and a more accurate assessment of bone loss using trial implants, the preparation of the proximal humeral allograft can commence. This involves making a cut at the anatomic neck of the allograft, just distal to the articular surface, which can be achieved using either a freehand technique or a cutting guide. Subsequently, the humeral canal is reamed and broached, ensuring the preservation of sufficient cancellous bone for cement fixation. Throughout this process, it is crucial to retain the tendon stumps on the allograft for a future repair to native tendons. An estimation of the required length of the allograft for reconstruction should be made preoperatively using radiographs with magnification markers. However, final adjustments regarding stem height and the size of the allograft should be made intraoperatively based on the total bone loss and soft-tissue tensioning. Once the necessary length of the allograft has been determined, the distal humeral cut is made, which may include a step cut to enhance torsional stability. To achieve compression at the graft–host junction, a 3.5-mm locking compression plate may be utilized in compression mode across the junction, ensuring the selection of a plate with sufficient holes proximal and distal to the junction. Otherwise, a cerclage wire at the site of the step cut may be employed to provide additional fixation (Fig. 7). Any preserved native tendons (such as the posterior cuff, deltoid, and pectoralis) should then be repaired to their respective allograft tendon stumps.
Fig. 7
Preoperative radiograph with an antibiotic-loaded spacer and postoperative radiograph of a revision shoulder prosthesis with allograft reconstruction
Revision reverse shoulder arthroplasty with a massive tumoral prosthesisWhile primarily employed in the oncologic setting for the wide resection of proximal humerus malignancies, a massive tumoral prosthesis can also be effectively utilized to address extensive bone defects. Surgeons often prefer this type of implant over osteoarticular allografts or allograft–prosthesis composites due to the latter's increased risk of nonunion and graft failure [14]. The highly modular design of these prostheses offers a relatively straightforward approach to restoring humeral length, and achieving an appropriate version is typically feasible through the use of the modular components. Native tendons can subsequently be reattached to the prosthesis using suture fixation, although the efficacy of soft-tissue healing to metal remains uncertain.
留言 (0)