In this secondary analysis of the EMERGE trial, the SGA rate was within population norms, with no statistically significant difference by metformin exposure. Our SGA rate (6.2%) was similar to that reported in the MiG trial (8.5%), which also investigated treatment with 2500 mg/day metformin [15]. Notably, the SGA rate was lower than that in the MiTy trial (11.8%), which included women with type 2 diabetes with/without complications, including nephropathy, and investigated a lower dose of metformin (2000 mg/day) [16]. However, notably, renal impairment or nephropathy was an exclusion criterion in the EMERGE study. Participants in the MiTy study also had a mean BMI of 35 kg/m2 compared with a mean BMI of 30 kg/m2 for the EMERGE participants.
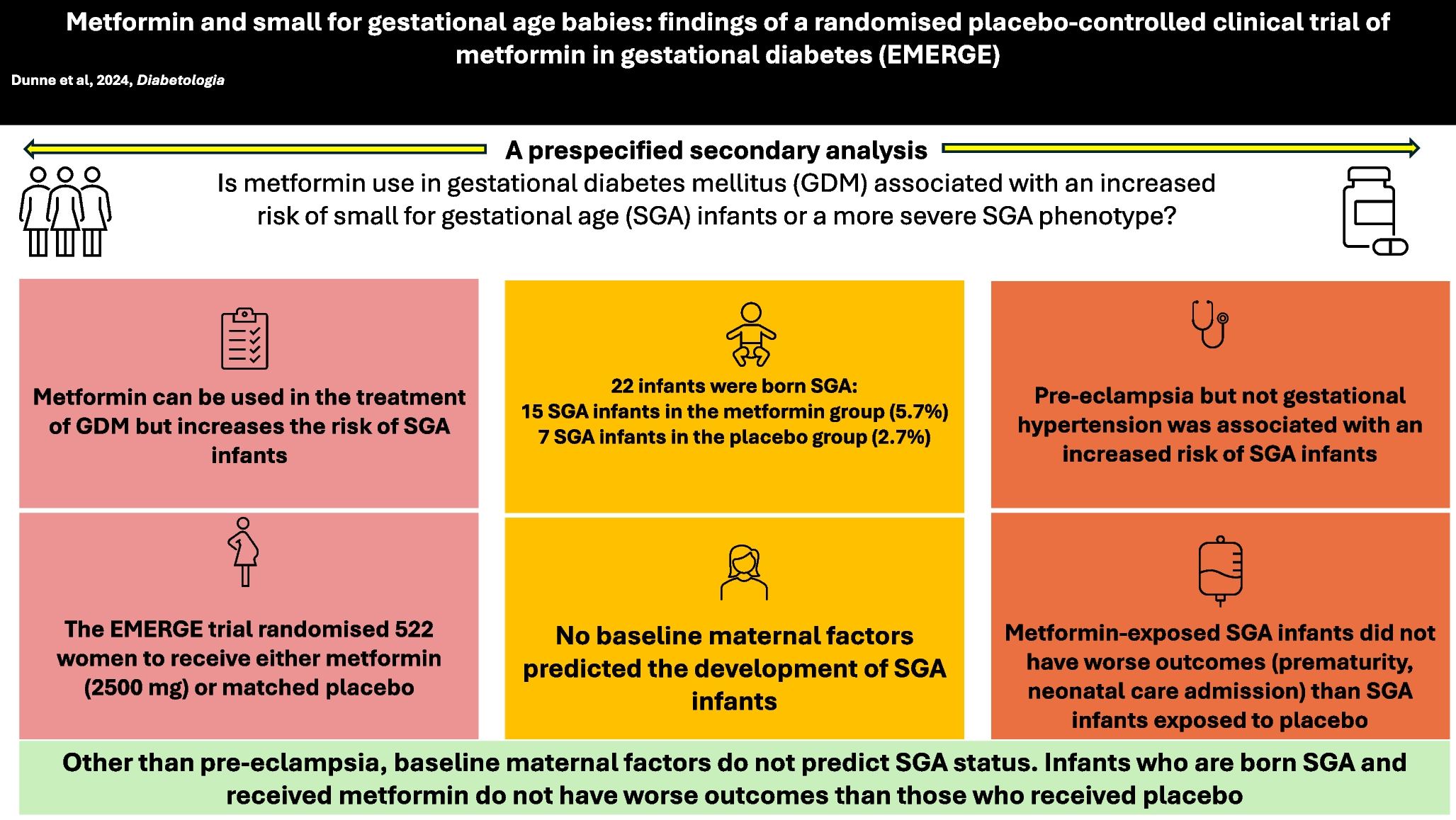
No baseline maternal factors were associated with an increased odds of having an SGA infant (univariate- or multivariable-adjusted analysis). As expected, SGA infant anthropometric measurements were lower than non-SGA infant measurements. Importantly, there were no statistically significant differences in neonatal outcomes by metformin exposure among SGA infants; however, some statistically non-significant differences may have clinical importance (e.g. lower birthweight and higher rate of jaundice in metformin-exposed individuals).
Maternal glycaemic management and insulin requirements were similar between those who did and those who did not have an SGA infant and were not associated with having an SGA infant. Pre-eclampsia and gestational hypertension were significantly associated with SGA infants on univariate analysis, and pre-eclampsia remained so after multivariable adjustment. Although the overall number of SGA infants was small, we found that metformin exposure did not increase the risk of pre-eclampsia and gestational hypertension in the SGA cohort. Taken together, these data suggest that hypertensive disorders of pregnancy may have a greater impact on SGA status in GDM pregnancies, with little impact of metformin.
In the EMERGE trial, metformin was introduced early following a GDM diagnosis, with participants randomised at a median of gestational week 27 and a median duration of treatment of 12 weeks, with no difference between the randomised groups. This differs from current routine practice in which metformin is not introduced until lifestyle treatment fails. Based on this secondary analysis, one would not expect an increase in SGA rates or a more severe SGA phenotype if metformin was introduced earlier in routine clinical practice.
This secondary analysis has several strengths. Data were derived from the EMERGE trial, a large, double-blind randomised trial comparing metformin with placebo in women with GDM, which had a low attrition rate and a high rate of adherence to treatment; in total, 98% of EMERGE pregnancies were included in this secondary analysis. This rigorous methodological approach allowed for a more focused examination of the specific research question while leveraging the high-quality data collected within a well-designed clinical trial framework. Furthermore, by carefully defining our inclusion criteria and using multivariable-adjusted regression analyses, we sought to minimise potential confounding factors and enhance the validity of our findings. This study also has limitations. We acknowledge that it may have been underpowered to detect associations; however, underpowered studies can still provide valuable insights and contribute to the overall body of knowledge in a given field. Although larger studies may be needed to confirm the results reported here, our study provides a valuable starting point for future research and highlights the need for continued investigation into the risk factors for SGA infants in the context of GDM and metformin exposure.
In conclusion, this secondary analysis of the EMERGE trial, although limited by the small sample size, found similar rates of SGA infants to previous trials, no significant increase in the odds of having an SGA infant with metformin and no statistically significant difference in maternal characteristics between those who did and those who did not have an SGA infant. The presence of hypertensive disorders of pregnancy was strongly associated with having an SGA infant, independent of metformin exposure.








留言 (0)