
記住我





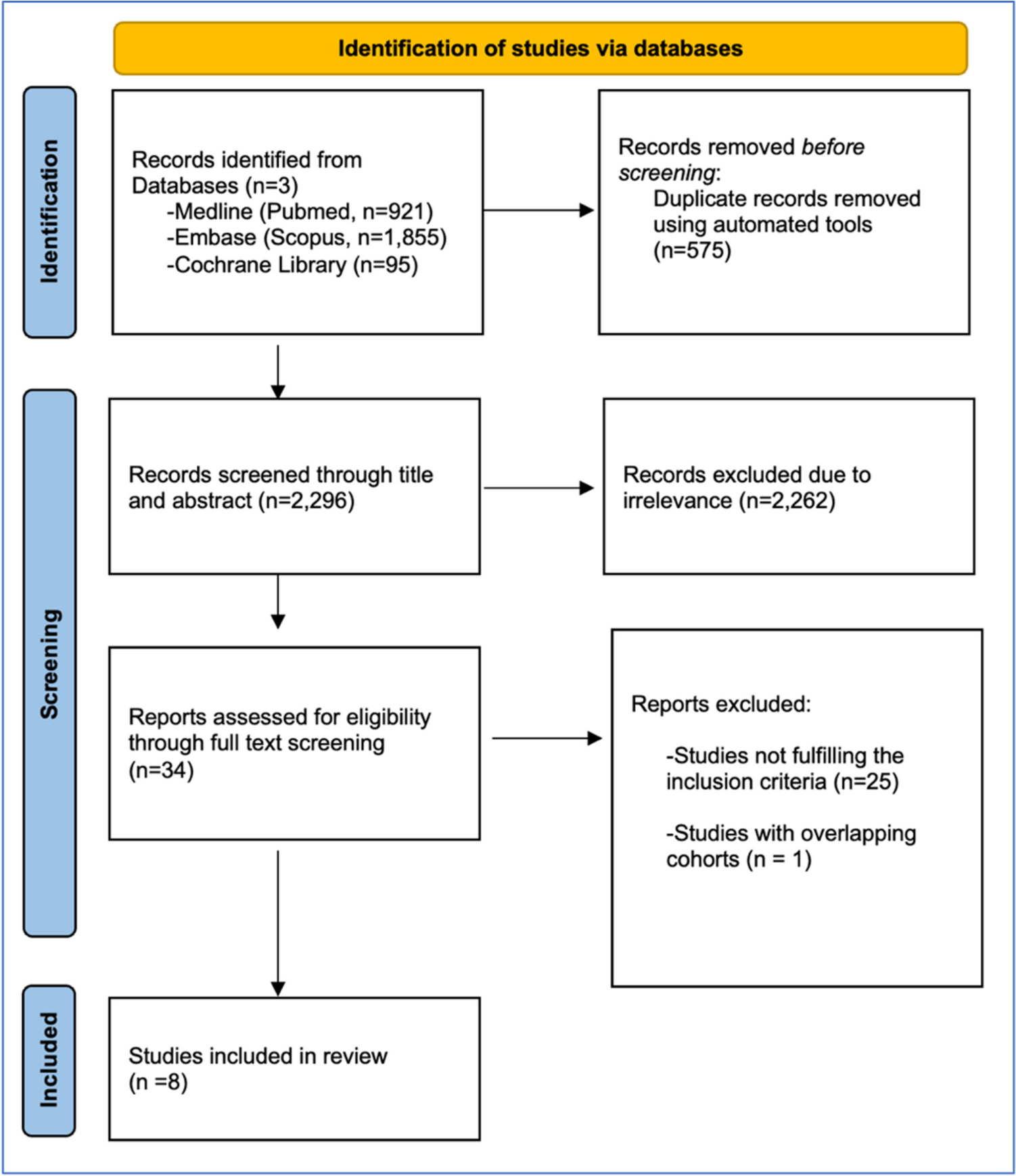

Figure 1 presents the flow chart of this systematic review. A total of 4467 records were identified and screened. After screening titles and abstracts, 64 full texts were assessed for eligibility. Twenty-four full texts were included, representing 20 original, individual studies conducted in gynecological cancer populations, of which 11 (55%) studies were RCTs (n = 1288 females), two (10%) were non-RCTs with two groups (n = 183 females), and seven (35%) were non-RCTs with single group (n = 230 females).
Fig. 1
Table 2 shows the characteristics of included studies. Studies are presented according to the study design (RCTs followed by non-RCTs), type of TG intervention (combined therapies followed by PFM and education-based therapies), arranged from the most recent to the oldest studies. The age range of females spanned from 32 to 66 years. The most represented gynecological cancer was cervical cancer, with 1326 females, representing 78% of gynecological cancer populations. One study (5%) examined a prehabilitation intervention (before cancer treatment), 10 (50%) rehabilitation interventions (after cancer treatment), and nine (45%) mixed interventions (delivery over more than one cancer treatment time phase). Full description of TG interventions as reported by the study authors and according to the TIDieR checklist can be found in Supplementary Information 2. The number of satisfied items from the TIDieR checklist, which was used to assess the quality of reporting of TG interventions, ranged between 5–11 (out of 12), representing 42%-92% of the total checklist items. Based on the available assessment timepoints in included studies, the majority used follow-up time frame related to short- and medium-term effectiveness, and only one study (5%) provided results for long-term effectiveness [10]. Studies reported intervention effect on bladder (n = 11, 55%), bowel (n = 6, 30%), vaginal (n = 6, 30%), overall pelvic floor (n = 2, 10%), sexual (n = 10, 50%), psychological (n = 8, 40%) function, quality of life (n = 8, 40%), and PFM function (n = 7, 35%).
Table 2 Characteristics of Included StudiesRisk of Bias and Quality AssessmentTables 3, 4 and 5 show the item and overall rating on the risk of bias or quality assessment tool of all included studies according to study design. For all RCTs, the overall risk of bias was assessed as ‘some concerns’ using the RoB tool. For non-RCTs with two groups, one study was of ‘poor quality’ and one of ‘fair quality’ according to the NOS. For non-RCTs with single group, the percentage of satisfied criteria ranged from 4 to 6 out of 7 on the JBI checklist. The agreement between reviewers for all scored items was 89%.
Table 3 RoB Domains of Reviewed RCTsTable 4 NOS Items of Reviewed Non-RCTs with Two Groups Table 5 JBI Checklist for Quasi-Experimental Study Items of Reviewed Non-RCTs with Single GroupOutcomesSupplementary Information 3 presents the findings of individual studies on bladder, bowel, vaginal, overall pelvic floor, sexual, psychological function, quality of life, and PFM function, along with considerations for interpretation. Only five studies out of the 20 included studies (25%) reported data on adverse events related to the TG intervention. Among these, one study reported no adverse events related to a PFM training program [36] and four studies reported temporary minor adverse effects experienced by a small number of participants [19, 20, 31, 34]. These included small amount of vaginal bleeding [34], irritation related to a vaginal product, and shoulder pain [31] for PFM therapies involving exercises with insertion of a device or dilator into the vaginal cavity, as well as urinary retention and dysuria for therapies involving catheterization [19, 20].
Bladder FunctionSix RCTs provided data on bladder function [18,19,20, 22,23,24], one of which presented results that were non-interpretable [24]. Based on two RCTs with reasonable sample sizes, PFM therapies (active or electrostimulation) reduced post-void residual (PVR) [19, 20]. An improvement in both urogenital distress (UDI-6) and urinary incontinence impact (UIQ-7) following a combination of PFM therapy (active) + education was found in another recent RCT (n = 130) [18], although a sample size calculation was not reported and some aspects of intervention dosage were unclear. Only one RCT identified a primary outcome which informed a sample size calculation (n = 40) [22], however the outcome selected was a post-intervention measure only, and no difference between groups was found following a combination of PFM therapy (active) + education with low supervision. An older RCT showed no difference between groups in bladder function (APFQ) following a combination of PFM therapy (active) + education + other exercises [23], however sample size was very small (n = 28) with no sample size calculation provided and the intervention appeared to be low intensity. Intervention descriptions were limited for the majority of RCTs.
One non-RCT reported findings from a two-group comparison indicating improvement in favor of TG for bladder emptying and bladder compliance outcomes (however the two groups were quite imbalanced in number: n = 76 for TG vs n = 44 for CG); but not for urethral closure pressure following PFM therapy (active + electrostimulation) [29]. Four studies reported results of single-group pre-post comparisons [10, 31, 34,35,36], ranging from very small (n = 8) to medium (n = 49) sample size. Among these, two studies stated a priori they were feasibility or pilot studies, and they achieved their pre-defined outcome indicating that the study or intervention was feasible [31, 34]. Three studies provided PFM (active ± passive) + education therapies, of which two demonstrated a significant improvement in bladder function (ICIQ-UI SF, pad test, 3-day bladder diary) from baseline to post-intervention [31, 35] and 12-month post-intervention [10], and one a non-significant improvement in bladder function (prevalence of urinary incontinence, ICIQ-UI SF) from baseline to post-intervention [34], although no studies were powered for these outcomes. One study did not show improvement in bladder function (ICIQ-UI SF) after PFM therapy (active) [36]; details of intervention were unclear, and the study had high attrition, whereas the other three studies [10, 31, 34, 35] reported their interventions clearly and attrition rates were lower.
Bowel FunctionThree RCTs provided data on bowel function [18, 23, 24]; results from one RCT were not interpretable [24] and the other two presented inconsistent findings [18, 23]. An improvement in both colorectal-anal distress (CRADI-8) and colorectal-anal impact (CRAIQ-7) following a combination of PFM therapy (active) + education was found in one recent RCT [18]. Even though this study had a reasonable sample size (n = 130) [18], no sample size calculation was reported and intervention reporting was limited in detail, as previously reported in the bladder function outcome results for this study. An older study that provided PFM therapy (active) + education + other exercises did not show a difference in bowel symptoms between groups [23], however, the very small sample size (n = 28) and more recent study may be factors in this negative finding.
Three studies reported results of single-group pre-post comparisons [31, 34, 36]. One study provided PFM (active ± passive) + education therapies and observed significant improvement in bowel function (ICIQ-B) [31], whereas another study showed non-significant improvement in bowel function (ICIQ-B and prevalence of fecal incontinence) post-intervention [34]; both followed the same direction of findings as for bladder function outcome. No improvement in prevalence of anal incontinence was found following PFM therapy (active) in the other study [36]; as mentioned in bladder outcome results, details of intervention were unclear, and the study had high attrition.
Vaginal FunctionThree RCTs provided data on vaginal function [18, 24, 26]. The most recent study identified an improvement in pelvic organ prolapse (POP) symptoms and impact (POPDI-6 and POPIQ-7) following PFM therapy (active) + education, although limitations of this study are as reported in bladder and bowel function outcome results above [18]. The other two RCTs, with n = 88 [24] and n = 318 [26], the latter corresponding to the largest study included in this review, investigated the effect of therapies including dilator therapy on vaginal stenosis and dimensions (instrument-measure outcome, LENT SOMA Scale); this was the primary outcome in Cerentini et al. [24]. Neither study detected a significant difference between groups. These results could have been affected by low adherence to the therapy [24], variation in vaginal dilator management among participants or lack of supervision, or timing of the intervention – during radiotherapy – in an heterogenous population [26], which may have made detection of a response to therapy difficult.
Three studies reported results of single-group pre-post comparisons [10, 31, 39, 40]. The study that provided a combination of PFM therapy (active + passive) + education [10, 31] demonstrated improvement in a range of vaginal signs and symptoms which were maintained 12-month post-intervention, with intervention details well reported. Two studies provided education interventions alone: psycho-education [39] and mindfulness-based cognitive behavioral intervention [40], neither of which showed improvement, and intervention descriptions were scant.
Overall Pelvic Floor FunctionOne recent RCT provided data on overall pelvic floor function [18]. This study showed a reduction in pelvic floor distress (PFDI-20) and impact on quality of life (PFIQ-7), which were listed as the primary outcomes for the study, following a combination of PFM therapy (active) + education [18]. Results followed the same direction of findings as for bladder, bowel, and vaginal function of the same study [18].
One two-group non-RCT provided PFM therapy (active + electrostimulation) and also showed a reduction in symptoms (pelvic floor distress [PFDI-20]) [29], supporting improvement observed in instrument-measured outcomes such as PVR, bladder compliance, and bladder detrusor systolic pressure [29]; but no primary outcome was stated. Intervention descriptions in both studies were scant.
Sexual FunctionFive RCTs provided data on sexual function [21, 23, 26,27,28]. Among these, two provided a combination of PFM therapy (active) + education + other, and both showed an improvement in sexual function (FSFI, APFQ), despite quite different sample sizes (n = 226 vs n = 28) [21, 23]; neither of these studies were powered for this outcome. Three RCTs provided education and findings were inconsistent [26,27,28]: one observed an improvement in sexual function (FSFI) (n = 69) [27], and the other two found no differences between groups (SVQ, Sexual History Form) (n = 318 and n = 32) [26, 28], of which one listed sexual function as the primary outcome [28]. The intervention dosage was either unclear [27] or low, and with high baseline outcome measure variance [26, 28]; follow-up timepoints were unclear [27, 28]; and one study included participants with different gynecological cancers who underwent radiotherapy during the study [26].
The only study that provided a sample size calculation based on a sexual function outcome was a non-RCT with two groups which provided an education-based intervention [30]. Although sample size was not achieved, the study found an improvement in sexual attitudes up to six weeks and sexual self-efficacy up to one week following the intervention [30]. Four studies reported results of single
留言 (0)