Our study shows how the integration of conventional testing with novel culture-independent systems and host-response technologies may increase our ability to diagnose persistent candidemia. Previous studies showed how T2 is more sensitive compared to conventional cultures. Specifically, the performance of the T2 on follow-up samples from an index episode of candidemia has been assessed by a large multicentre trial showing how T2 was more likely to be positive than BC in patients receiving antifungals [4]. Similarly, the STAMP trial assessed the role of T2 for monitoring the clearance of candidemia, again showing how only 30% of positive T2 follow-up samples were accompanied by positive BCs [5], and in-vitro studies also confirmed how the T2 performance is not affected by the inoculation of antifungals into BC vials [10]. A preliminary report subsequently suggested that T2 may be able to predict adverse outcomes in patients with proven candidemia [11]. Nonetheless, whether the persistence in the bloodstream of fungal DNA rather than of live culturable microorganisms, may have clinical and prognostic significance is yet to be confirmed in large studies.
Our results confirm a higher positivity rate of T2 compared to BC on follow-up samples of a small group of patients with candidemia. Nonetheless, we also detected some BC+/T2– results highlighting how T2 false negative results exist. One of the two T2+/BC negative discordant cases we detected, may be explained by the delayed collection of the T2 sample compared to the BC, due to logistic delays in the ward. All other daily blood collections were however performed within the same draw. The T2 false negative results highlight the limitations in the accuracy of the T2 technology, suggesting caution in using T2 results to rule out infection or support early step-down of antimicrobials, but rather highlighting its usefulness in combination with, rather than in place of, conventional BCs. A high rate of invalid results was also observed in our study (3/34, 9%), possibly due to the use of frozen rather than fresh samples.
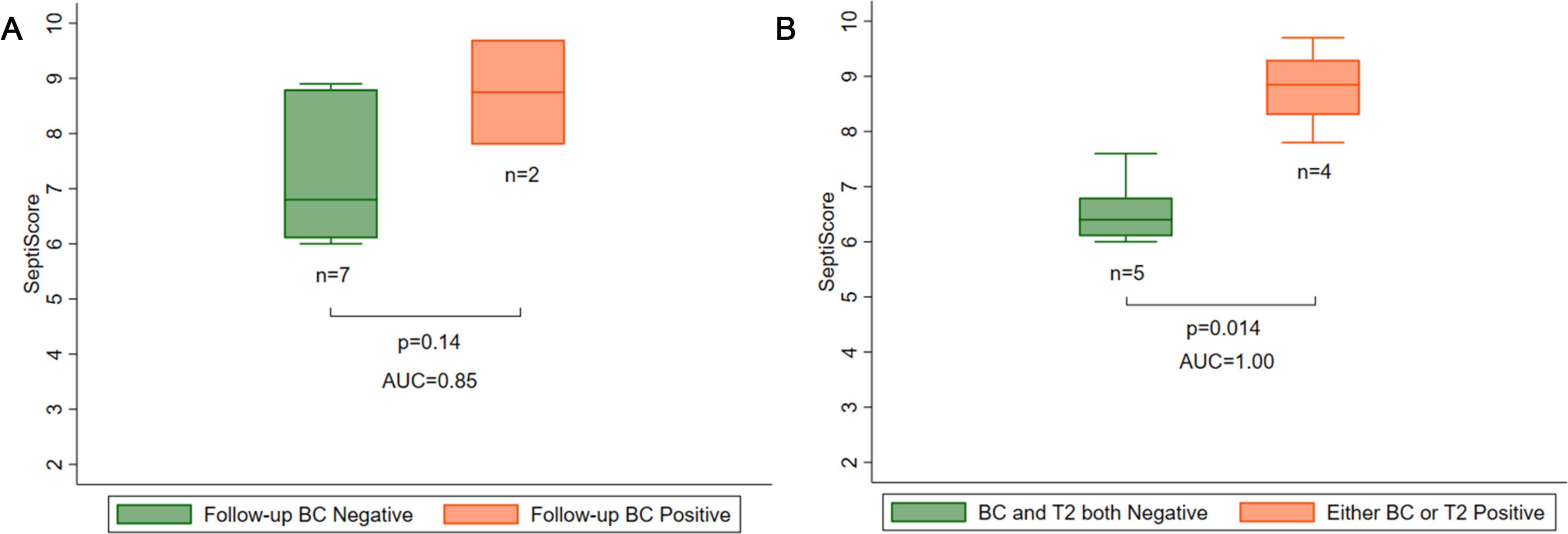
Given the limitations of conventional cultures in diagnosing candidemia [3] and in the perspective of exploiting synergism between novel and conventional diagnostic approaches, we investigated whether SeptiScore could also support clinicians to this scope. Interestingly, SeptiScore showed a better performance in predicting persistent candidemia when this was defined according to either T2 or BC positivity, compared to when persistent candidemia was defined by the use of BC only. This suggests how patients with persistently positive T2 samples in the context of an episode of candidemia may have a high host inflammatory response as measured by the SeptiCyte, again supporting the interpretation of the “T2emia” as a true BSI rather than as the mere persistence of fungal DNA lacking clinical significance, or a false positive result. At the same time, our results suggest a potential use of SeptiScore for detecting persistent candidemia, with higher performance when used in combination with both conventional cultures and novel culture independent testing rather than in association with conventional systems only. Future studies on larger samples size may clarify the performance of this integrated diagnostic approach and its potential clinical applications.
Overall, our observations open interesting research questions on the opportunity of redefining our current gold standard for the diagnosis of candidemia, and of BSI in general, in an era of rapidly evolving diagnostics. Both culture independent microbiological techniques, and the omics technologies have the potential to transform the diagnostic approach to BSI and sepsis [12].
Our study has several limitations. Firstly, it was a preliminary clinical observation on a very small sample size. Secondly, our definition of persistent candidemia was based on results of single days. However, some patients had intermittent positivity of BC or T2 over the 4 days of follow-up and whether to interpret negative BC/T2 results before a new positivity as true negatives may be questionable. Indeed, we could argue that the clearance of the bloodstream had not happened yet, although the possibility of intermittent candidemia still exists. Thirdly, none of our patients were diagnosed with metastatic infection, so we were unable to explore any association between SeptiScore and metastatic dissemination of candidemia. A fourth limitation pertains to our classification of T2 invalid results as negative when candidemia was diagnosed based on results of both BC and T2. Lastly, we built ROC curves at day 1 only because that day had the highest number of positive results for both tests.
In conclusion, our study suggests how utilising both conventional culture and culture-independent systems may enhance diagnosis of persistent candidemia. Further studies are needed to clarify the role of transcriptome profiling for the diagnosis of candidemia and how this could be integrated with microbiological testing to improve patients’ outcomes.







留言 (0)