
記住我
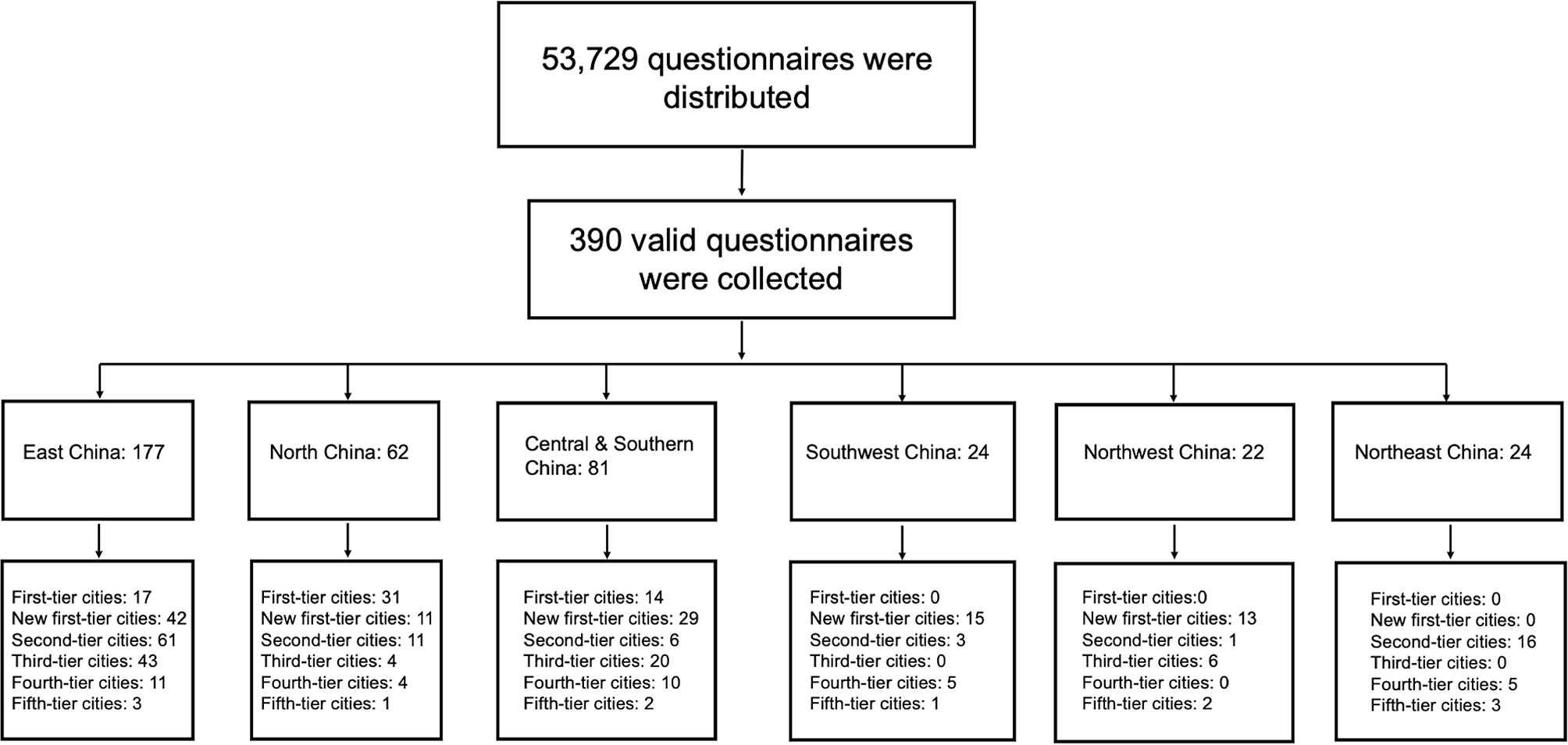




A total of 53,729 questionnaires were distributed and 390 valid questionnaires from 319 hospitals located in 124 cities around China were collected between December 9, 2022 and March 6, 2023. 94.1% (n = 367) of the surveyed physicians were from grade A tertiary hospital and 82.3% (n = 321) of them were from general hospital. 59.0% (n = 230) were from department of oncology and 32.6% (n = 127) were from department of respiratory medicine. The characteristics of participating physicians including city tier, hospital type and departments are shown in Table 1.
Table 1 Basic characteristics of 390 physicians with valid questionnairesAmong the 124 cities, 18 were first-tier/ new first-tier cities, accounting for 95% of all 19 first-tier/ new first-tier cities; 28 were second-tier cities, accounting for 93% of all 30 second-tier cities; and 78 were third or lower-tier cities, accounting for 27% (78/288) of all such cities [28]. Detailed region distribution of the 390 questionnaires is shown in Fig. 1.
Fig. 1
Region distribution of the 390 questionnaires collected in this study. Note: The first-tier cities: Beijing, Shanghai, Guangzhou, Shenzhen; The new first-tier cities: Tianjin, Chongqing, Hefei, Foshan, Zhengzhou, Wuhan, Changsha, Nanjing, Suzhou, Qingdao, Xi’an, Chengdu, Hangzhou, Ningbo; The second-tier cities: Fuzhou, Quanzhou, Xiamen, Lanzhou, Huizhou, Zhongshan, Nanning, Guiyang, Baoding, Shijiazhuang, Harbin, Changchun, Changzhou, Nantong, Wuxi, Xuzhou, Nanchang, Dalian, Shenyang, Jinan, Linyi, Weifang, Yantai, Taiyuan, Kunming, Jinhua, Shaoxing, Wenzhou; The third-tier cities: Anqing, Fuyang, Wuhu, Ningde, Putian, Zhangzhou, Chaozhou, Qingyuan, Shantou, Zhanjiang, Guilin, Liuzhou, Haikou, Lang fang, Tangshan, Kaifeng, Luoyang, Nanyang, Xinxiang, Jingzhou, Yueyang, Zhuzhou, Huai’an, Taizhou, Yancheng, Zhenjiang, Ganzhou, Jiujiang, Shangrao, Hohhot, Yinchuan, Heze, Jining, Liaocheng, Weihai, Zibo, Xianyang, Urumqi, Huzhou, Taizhou; The fourth-tier cities: Bozhou, Huaibei, Huangshan, Tongling, Maoming, Baise, Chengde, Jiaozuo, Pingdingshan, Shiyan, Xiaogan, Huaihua, Loudi, Yiyang, Jilin, Dandong, Jinzhou, Baotou, Binzhou, Dongying, Zaozhuang, Jinzhong, Linfen, Dazhou, Leshan, Neijiang, Yibin; The fifth-tier cities: Wuwei, Qinzhou, Jingmen, Siping, Pingxiang, Xinyu, HuLudao, Liaoyang, Hulunbuir, Zigong, Shihezi
The survey outcome revealed that the 390 participants on average treated approximately 10 patients with advanced EGFR exon20ins-mutant disease every 6 months, which accounted for 3.8% of all advanced NSCLC patients they were treating during the same period, and there was no significant difference between departments (data not shown).
Overall status of the diagnosis and treatment of patients with EGFR exon20ins-mutant NSCLCThe rate of EGFR mutation tests and testing methodsPhysicians reported that among patients with advanced NSCLC receiving first- or second-line treatment, 80.9% and 59.9% underwent EGFR mutation tests, respectively, and there was no significant difference in the testing rate across different departments (data not shown). In the first-line setting, 25.0% (98/390) of the surveyed physicians reported a 100% EGFR testing rate. Among the remaining physicians (292/390, 75.0%) who did not reach a 100% EGFR testing rate, the reasons for not performing EGFR testing (based on a multiple-choice question) included patient-related factors (financial considerations and personal willingness, 224/292, 76.7%), patients who were pathologically confirmed to have squamous cell carcinoma (185/292, 63.4%), patients who had already undergone an EGFR mutation test elsewhere prior to the current hospital visit (115/292, 39.4%), and patients with insufficient tumour tissue samples (112/292, 38.4%) (Figure S1A).
With respect to EGFR mutation test methods in first-line setting, NGS was performed for 75.0% of the patients, including 62.0% performed NGS test only and 13.0% performed NGS plus PCR dual test. For the additional question concerning EGFR mutation test methods in first-line that 270 physicians answered, 21.9% (59/270) reported using the NGS method exclusively for EGFR testing. Among the remaining 78.1% (211/270) who did not achieve a 100% NGS testing rate, the following reasons for not performing NGS testing (based on a multiple-choice question) were provided: patient-related factors (financial consideration or personal willingness) (184/211, 87.2%), insufficient/low-quality tumour tissue samples (112/211, 53.1%), unavailability of in-house NGS tests (75/211, 35.5%), and long NGS testing duration (64/211, 30.3%) (Figure S1B). The proportion of patients who did not receive the NGS test due to the unavailability of the test was greater in third- or lower-tier cities than first-tier cities (27.2% in first-tier cities vs. 49.3% in third- or lower-tier cities, p < 0.05) (data not shown).
Physicians’ general understanding of the EGFR exon20ins mutationPhysicians’ comprehension of the EGFR exon20ins mutation was assessed via a series of questions related to the characteristics of the EGFR exon20ins mutation, subtypes of the mutation, mutation insertion locations, and the effectiveness of 1st -3rd generation EGFR-TKIs.
Among 390 surveyed physicians, 85.9% (n = 335) were aware that EGFR exon20ins was a primary driver mutation, but 14.1% (n = 55) of the surveyed physicians considered EGFR exon20ins a secondary drug-resistant mutation (Fig. 2A). The percentages of surveyed physicians who knew that EGFR exon20ins mutations occurred in the αC-helix and postαC-helix loops were 77.9% (304/390) and 80.3% (313/390), respectively (Fig. 2B). Regarding the subtypes of the mutation, 70.0% (273/390) and 67.4% (263/390) of the surveyed physicians correctly identified p.767_V769dup and H773_V774insNPH as subtypes of the EGFR exon20ins mutation (Fig. 2C). Furthermore, 37.4% (146/390) of the surveyed physicians knew that the 1st -3rd−generation EGFR TKIs were effective against the A763_Y764insFQEA subtype (Fig. 2D).
Fig. 2
The results of questions concerning physicians’ understanding of EGFR exon20-ins mutations (n = 390). A. Is EGFR exon20ins mutation a primary mutation or an acquired drug-resistance mutation? (single-choice); B. Where do EGFR exon20in mutations occur? (multiple-choice); C. Which are EGFR exon20ins mutations? (multiple-choice); D. Which one of the following subtype is sensitive to 1st -3rd generation EGFR TKIs? (single-choice). EGFR, epidermal growth factor receptor; TKI, tyrosine kinase inhibitor
Current clinical practices in the treatment of patients with EGFR exon20ins-mutant NSCLCIn the case of patients with EGFR exon20ins-mutation undergoing first-line treatment, the three most commonly used regimens included chemotherapy combined with antiangiogenic therapy (30.0%), 1st -3rd -generation EGFR-TKI monotherapies or EGFR-TKI-based combinations (18.3%), and chemotherapy alone (16.8%). For patients receiving second-line therapies, the three most commonly used regimens were chemotherapy combined with antiangiogenic therapy (25.0%), chemotherapy alone (18.5%), and chemotherapy combined with ICIs (16.4%). In addition, 11.9% and 15.7% of patients on first-line or second-line treatment, respectively, received novel EGFR exon20ins-targeted therapies (including TKIs and bispecific antibodies) (Fig. 3A).
Fig. 3
A. Proportions of physicians using first-line and second-line therapy in EGFR exon20ins-mutant patients. B. Physicians’ scaling scores for the efficacy and safety of each therapy. Notes On a scale of 1–7, a score of 1 indicates the lowest level of satisfaction, and a score of 7 indicates the highest level of satisfaction. * ICI-based combination therapies, including ICI + chemo + VEGF(R)i, ICI + VEGF(R)i, etc. **1st -3rd generation TKI alone or in combination. *** EGFR exon20ins-targeted agents include TKIs and bispecific antibodies. Chemo, chemotherapy; VEGF(R)i, vascular endothelial growth factor (receptor)-targeted inhibitor; ICI, immune checkpoint inhibitor; EGFR, epidermal growth factor receptor; Gen, generation; TKI, tyrosine kinase inhibitor
Physicians’ overall perspectives on treatment optionsPhysicians’ views on existing treatment optionsA total of 278 physicians answered additional questions on first-line treatment, with 74.8% (208/278) had prescribed novel targeted agents. 270 physicians answered questions on second-line treatments, with 76.7% (n = 207) prescribed novel targeted agents.
To further understand the unmet need in the treatment of patients with the EGFR exon20ins mutation, this study assessed physicians’ views on the overall efficacy and safety of existing treatment options. Regardless of the line of treatment, novel EGFR exon20ins-targeted agents (including TKIs and bispecific antibodies) received the highest score in terms of satisfaction (first-line: 5.3/7; second-line: 5.3/7), followed by the most commonly used chemotherapy plus antiangiogenic therapy (first-line: 4.8/7; second-line: 4.4/7) (Fig. 3B).
Compared to physicians who had never prescribed novel targeted therapies, those physicians who had ever prescribed novel targeted therapies had higher satisfaction scores (first-line: 5.5/7 vs. 4.8/7; second-line: 5.4/7 vs. 4.6/7) (Figure S2A). Moreover, EGFR exon20ins-targeted TKI ranked the most promising therapy both in first line and second-line and beyond setting in the future regardless of the prescription history of physicians. (Figure S2B)
With respect to the safety profile, regardless of the treatment line, the three highest satisfaction scores were given to novel EGFR exon20ins-targeted agents (including TKIs and bispecific antibodies) (first-line: 5.3/7; second-line: 5.2/7), 1st -3rd generation EGFR TKIs as monotherapies or in combination (first-line: 5.1/7; second-line: 4.8/7), and chemotherapy plus antiangiogenic therapy (first-line: 4.7/7; second-line: 4.4/7) (Fig. 3B).
Physicians’ views on targeted therapy for the treatment of patients with EGFR exon20ins-mutant NSCLCMost physicians, regardless of their experience in prescribing novel targeted therapies, considered EGFR exon20ins-targeted TKIs the most promising treatment strategy for patients with EGFR exon20ins-mutant NSCLC (first-line: 223/278, 80.2%; second-line: 198/270, 73.3%) (Fig. 4A). When all of the given novel EGFR exon20ins-targeted agents were considered, sunvozertinib received the highest recognition for efficacy and safety (126/390, 33.2% and 126/390, 33.2%), followed by mobocertinib (110/390, 28.9%) and 109/390, 28.7%) (Fig. 4B).
Fig. 4
Physicians’ views on the most promising therapy for EGFR exon20ins-positive patients (A), and the novel targeted agents with the highest efficacy and best safety (B). *1st -3rd generation TKI alone or in combination. ** ICI-based combination therapies, including ICI + chemo + VEGF(R)i, ICI + VEGF(R)i, etc. EGFR, epidermal growth factor receptor; TKI, tyrosine kinase inhibitor; BsAb, bispecific antibody; ICI, immune checkpoint inhibitor; Combo, combination; Chemo, chemotherapy; VEGF(R)i, vascular endothelial growth factor (receptor)-targeted inhibitor
The most important indicators for physiciansThis study revealed that overall survival (OS) (297/390, 76.2%), progression-free survival (PFS) (225/390, 57.7%), and safety (214/390, 54.9%) were regarded by physicians as the most important clinical indicators for evaluating novel targeted agents. In comparison, the convenience of drug administration (64/390, 16.4%) and mechanism of action (72/390, 18.5%) were considered less important (Fig. 5).
Fig. 5
The most important indicators for physicians in choosing novel targeted agents. OS, overall survival; PFS, progression-free survival; ORR, objective response rate; AEs, adverse events
留言 (0)