This retrospective cohort study was performed in two level one trauma centers in Switzerland; Inselspital, University Hospital of Bern and Hospital of Canton St. Gallen (KSSG). The study protocol was approved by the local cantonal ethics committee of the Canton of St. Gallen (approval EKOS 23/178, project number 2023-01801). This report follows the applicable STROBE guidelines [16].
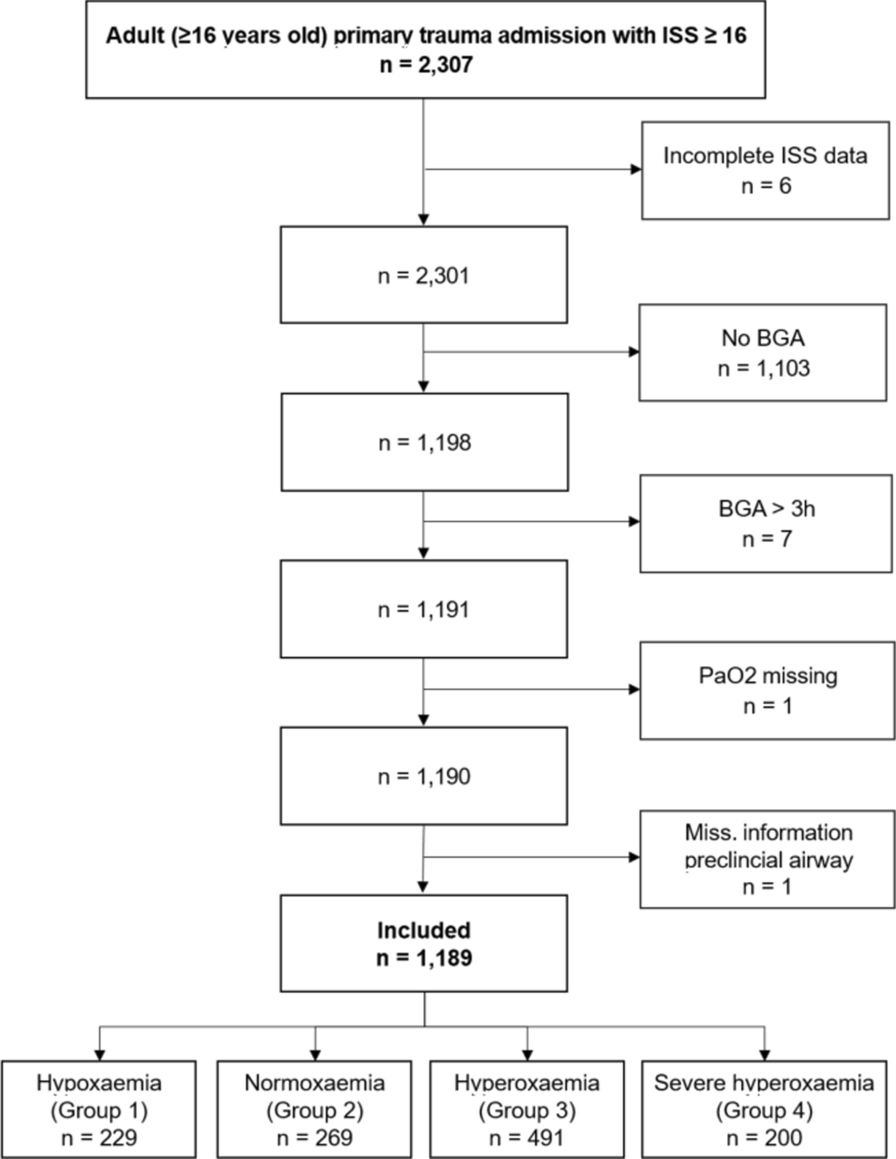
Anonymized patient data from the electronic health records in both hospitals were screened for all patients that presented to Inselspital Bern or KSSG for acute trauma care between 01.01.2017 and 31.12.2022. Screening included coding of free text data through standard trauma scoring systems such as Injury Severity Index (ISS) [17, 18] and abbreviated injury scale (AIS) [19]. Inclusion criteria were primary admission with trauma and ISS ≥ 16, age ≥ 16 years old, and arterial blood gas analysis (aBGA) performed within 3 h after admission. Exclusion criteria was missing PaO2 (arterial partial pressure of oxygen) value in the initial aBGA and missing information on prehospital airway status (intubated or not). Severe trauma to a specific body region was defined as having a maximum AIS of three or higher for that region.. Demographic data, pre-hospital and clinical data as well as details on injury were collected.
Based on the first available result of PaO2 within the first 3 h after admission, patients were divided into four groups [20]:
Group 1 hypoxaemia: all patients with PaO2 < 10.7 kPa (80 mmHg)
Group 2 normoxaemia: all patients with PaO2 between 10.7 and 16.0 kPa (80–120 mmHg)
Group 3 mild hyperoxaemia all patients with PaO2 above 16.0 to 40 kPa (120–300 mmHg)
Group 4 severe hyperoxaemia: all patients with PaO2 above 40 kPa (300 mmHg)
Normoxaemic patients (group 2) served as reference group. Demographic data, pre-hospital and clinical data and injury scores were calculated and compared for all four groups.
Statistics
As primary outcome, 28-day mortality was assessed and compared across groups, with group 2 (normoxaemia) as reference. For secondary outcomes, length of ICU stay (LOS-ICU) and length of hospital stay (LOS) were calculated and compared between groups. A predefined set of complications (stroke, myocardial infarction, pulmonary embolism, deep vein thrombosis, pressure ulcer, renal insufficiency, abdominal distension, wound infection, pneumonia, urinary tract infection, sepsis, compartment syndrome (extremity), abdominal compartment syndrome, acute lung injury (ALI) / acute respiratory distress syndrome (ARDS), cardiac arrest, multiorgan failure) were reported.
Data were analyzed with STATA 18.1 (StataCorp, College Station, TX, USA). For primary and secondary endpoints, odds ratios (OR) were calculated in addition to 95% confidence intervals for all point estimates. Depending on normality testing (Shapiro Wilk) median (interquartile range (IQR)) respectively mean (standard deviation (SD)) are shown for continuous variables, p-values obtained by Kruskal–Wallis test (for more than two groups) or Wilcoxon rank sum test (for two groups). Categorical variables are shown with number (%) in each category, p-values obtained by Chi-squared test. No p-value adjustment was performed.
Baseline data was used to derive a multivariable logistic (linear) regression model for the association between the four oxygen groups and the primary (secondary) endpoint as follows:
If binary variables were based on present continuous variables (such as hypotension on systolic blood pressure), the continuous parameter was used only to derive to the final model to avoid collinearity. Furthermore, oxygen saturation and GCS were not included in the multivariable model based on collinearity testing with oxygen group respectively AIS head (Variance Inflation Factor of > 2.5). Missing values were imputed and a stepwise backward regression analysis with a p-value of 0.05 was used to get to the final model. Oxygen group was forced in the final model. Logistic regression associations were presented as adjusted OR (aOR), linear regression associations with the coefficient accompanied with a 95% confidence interval (CI). Last, to explore non-linear associations of PaO2 and 28-day mortality, a fractional polynomial regression was used in one dimension with different powers (− 2, − 1, − 0.5, 0 = ln, 0.5 1, 2, 3) adjusted for the same co-variables as the final model. The proposed model was visualized with an adjusted predicted probability plot.
With a total of an expected 1200 trauma patients (around 200 patients per year), with 300 patients in each of the four oxygen groups, we would have been able to detect a clinical meaningful difference of 7% in 28-day mortality between normoxaemia (14%) and severe hyperoxaemia (21%).






留言 (0)