Study design
A retrospective multicenter observational cohort study, the Activation of Coagulation and Inflammation in Trauma-2 (ACIT-2) study [6]. Patients were excluded from the study if they arrived > 2 h post-injury; were transferred from another hospital; received more than 2000 ml crystalloid pre-hospital; or had sustained burns of over 5% of their body surface area. Pre-hospital tranexamic acid and/or blood product transfusion prior to hospital arrival was allowed. Patients were retrospectively excluded if they declined to give consent to the use of their research samples, had severe liver disease, a known pre-existing bleeding diathesis, or were taking anticoagulant medication (excluding aspirin) pre-injury.
Patient characteristics
313 out of 2019 patients were included from the ACIT study recruited between January 2008 and July 2014, all adults (≥ 18 years old) and moderately to severely injured (Injury Severity Score (ISS) ≥ 16), who had endothelial biomarker data (syndecan-1, soluble thrombomodulin, and adrenaline) and measurements of 13 selected single nucleotide polymorphisms (SNP) of the β2-adrenergic receptor, thrombomodulin, endothelial protein C receptor (EPCR), heparanase, E-selectin and Fibrinogen. The availability of SNP´s determined the number of patients included.
Research personnel at each center screened and enrolled patients. Data were collected prospectively and included patient demographics, time of injury, mechanism of injury (blunt or penetrating), TBI (AIS Head > 3), ISS, vital signs on-scene and on arrival in the emergency department, total number of blood products, and volume of intravenous fluids administered within the first 12 h from injury. Patients were observed for 28 days from injury for the occurrence of venous thromboembolic events (deep vein thrombosis or pulmonary embolism), and overall mortality.
Blood sampling
The blood samples were drawn within 20 min of the patient’s arrival in the emergency department including prothrombin time (PT), INR, arterial blood gas analysis.
For thromboelastometry (ROTEM®) analysis, a 2.7 ml citrated vacutainer (0.109 Molar/3.2% sodium citrate; Becton, Dickinson and Company, Plymouth, UK) was collected. Blood for coagulation and fibrinolysis protein assays was collected in a 4.5 ml glass citrated vacutainer (0.109 Molar/3.2% sodium citrate; Becton, Dickinson and Company, Plymouth, UK). The filled 4.5 ml vacutainer was centrifuged within 1 h of collection, and double-spun plasma subsequently stored at − 80 °C.
Viscoelastic hemostatic analyses
Functional hemostatic analysis was performed within one hour of blood draw at 37 °C on a ROTEM® delta instrument (Tem International GmbH, Munich, Germany) using the automated electronic pipette according to the manufacturer’s instructions. The methodology and parameters of ROTEM® have been described previously [16].
Biomarkers of SHINE, coagulation, and fibrinolysis
Plasma stored at − 80 °C was thawed to 37 °C immediately before all analyses. The soluble biomarkers adrenaline, syndecan-1, soluble thrombomodulin, E-selectin and VE-cadherin were measured by commercially available immunoassays according to the manufacture’s recommendations. Adrenaline (2-CAT ELISA, Labor Diagnostica Nord GmbH & Co. KG, Nordhorn, Germany; lower limit of detection (LLD) 10 pg/mL (adrenaline, normal reference < 100 pg/mL), Syndecan-1 (Diaclone Nordic Biosite, Copenhagen, Denmark; LLD 4.94 ng/mL), soluble thrombomodulin (Nordic Biosite, Copenhagen, Denmark; LLD 0.31 ng/mL), soluble E-selectin (IBL International GMBH, Hamburg, Germany; LLD 0.3 ng/mL) and soluble VE-cadherin (R&D Systems Europe, Ltd., Abingdon, UK; LLD 0.113 ng/mL).
An automated analyzer (Sysmex CA-CS100i System; Siemens AG) analyzed the following coagulation factor activities (normal range): Factor II (FII: 0.78–1.17 IU/mL), factor V (FV: 0.66–1.14 IU/mL), factor VII (FVII: 0.150–1.50 IU/mL), factor VIII (FVIII: 0.52–1.53 IU/mL), factor IX (FIX: 0.58–1.38 IU/mL), factor X (FX: 0.50–1.50 IU/mL), factor XI (FXI: 0.50–1.50 IU/mL), factor XIII (FXIII: 0.70–1.40 IU/mL), vW antigen (vWF Ag: 0.50–1.60 IU/mL), protein C (PC: 0.75–1.34 IU/mL), antithrombin (AT: 0.80–1.30 IU/mL).
Prothrombin fragment 1 + 2 (PT Frag 1 + 2; Enzygnost® F 1 + 2 (monoclonal); Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany), tissue plasminogen activator (tPA; Asserachrom® tPA, Diagnostica Stago, Asnières sur Seine, France), plasminogen activator inhibitor-1 (PAI-1; Asserchrom® PAI-1; Diagnostica Stago), plasmin-α2-antiplasmin complex (PAP; PAP micro ELISA; DRG Instruments GmbH, Marburg, Germany), urokinase (uPA, Abcam, UK) (Abbexa, Cambridge, UK) were measured using sandwich enzyme-linked immunosorbent assays (ELISAs). Fibrinogen levels (Siemens Thrombin reagent, Sysmex UK) and α2-antiplasmin (Siemens Berichrom α2-antiplasmin; Sysmex UK) were determined in the hospital laboratories with a Sysmex CS2100i automated analyzer (Sysmex UK) according to standard protocols. Latex immunoassays were used to quantify the levels of D-dimer (Siemens Innovance D-dimer; Sysmex UK) also with the Sysmex CS2100i automated analyzer.
SNP analyses
DNA was isolated from buffy-coat by QiaGen FlexiGen protocol and it was screened by means of a multiplex TaqMan-based analysis on a Via7 instrument (Applied Biosystems). Single Nuclear Polymorphism (SNP) assays of the β2-adrenergic receptor: Rs 1,042,713; Rs 1,042,714; Rs 1,042,717; Rs 1,800,888, thrombomodulin: Rs 1962; Rs 1,042,580; Rs 3,176,123, endothelial protein C receptor (EPCR): Rs 867,186, heparanase: Rs 4,364,254; Rs 4,693,608, E-selectin: Rs 1,805,193; Rs 5361 and Fibrinogen: Rs 2,020,918 that were validated on 10 samples each by direct sequencing of PCR products before analyses. The SNP´s focused on the glycocalyx, the protein C system, the sympathetic adrenergic system which are the parts of SHINE and E-selectin, an activation marker of the endothelium, together with fibrinogen, which is a pivotal part of TIC.
SHINE phenotypes
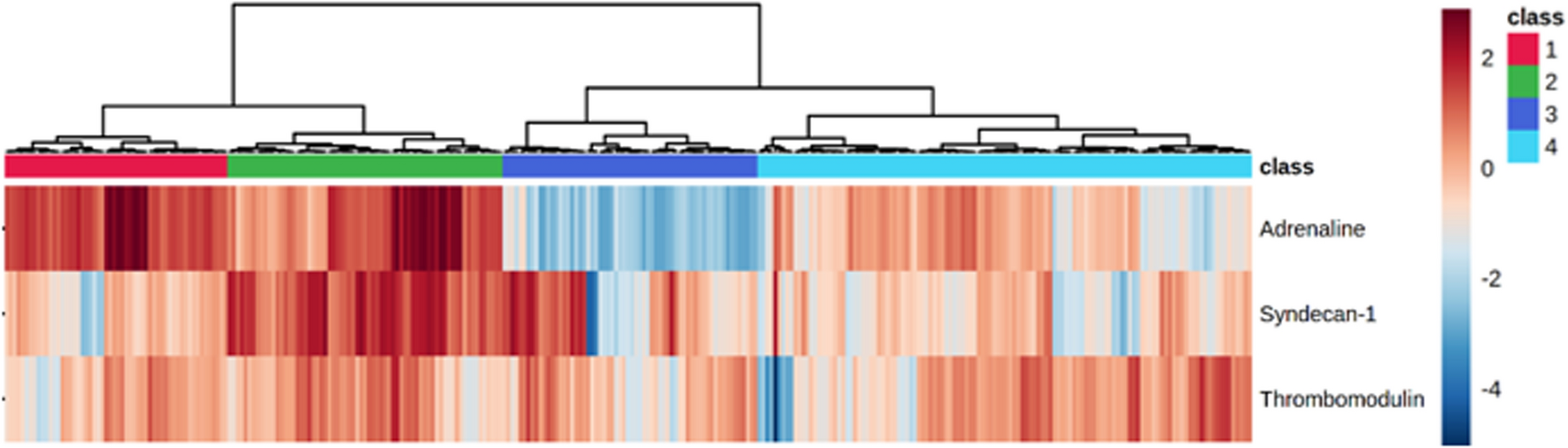
The SHINE phenotypes were developed using the biomarkers adrenaline, syndecan-1, and sTM, reflecting the level of sympathetic activation, degree of glycocalyx damage and severity of impairment of the protein C system, as previously described [7]. The data was converted to ng/ml and normalized by log2 and further Pareto scaled before creating a heatmap with an unsupervised hierarchical clustering algorithm using a dendrogram with the Euclidian distance measure and the ward cluster algorithm.
In total, 11 patients had an adrenaline value below LLD and were considered missing values, i.e., 3.5% of the total population. To handle this, a random forest imputing approach was applied on the datafile of all measured biomarkers (adrenaline, noradrenaline, syndecan-1, sTM, sE-selectin, and VE-cadherin) using Missforest package in R [17], allowing a minimally altering of the biomarker characteristics.
Statistical analyses
Statistical analyses were performed in RStudio 2022.07.1. Group characteristics and biomarkers were compared by Kruskal–Wallis test or Pearson Chi-Square test with unadjusted p-values reported. Post-hoc pairwise comparisons were done by Kruskal–Wallis test or Fisher’s test, adjusted for multiple testing by the Holm-Bonferroni method. Adjusted p-values < 0.05 were considered significant.
Analysis of the 20 measured pro -and anti-coagulation -and fibrinolytic factors contribution to the SHINE phenotypes was assessed by partial least squares-discriminant analysis (PLS-DA) to identify the importance of the variables among the phenotypes (VIP score). In total, 6.2% of features were missing the coagulation biomarkers data set. Missing values were imputed using the Missforest package in R and were log2, and Pareto scaled prior to the PLS-DA analysis.






留言 (0)