
記住我





Multiple MIO techniques for different anatomic regions have been described in the literature, including extensive reviews discussing its advantages and risks [8, 10, 14, 16, 18, 22,23,24,25,26,27,28]. Minimal invasive surgery has become widely accepted in all types of disciplines, ranging from visceral to orthopedic surgery [1,2,3]. New instruments permit percutaneous surgery for the spine and pelvis [29,30,31,32,33]. Nevertheless, to our knowledge, an attempt to generalize an algorithm with guidelines for MIO approaches has not been established yet.
The following considerations for any surgical approach to carry out an MIO need to be taken into consideration. The applied approach should include: A successful fracture reduction with instruments, adequate plate positioning and locking, as well as minimal damage to anatomical structures and tissues.
The surgical approach itself for articular fractures is placed directly onto the fracture and its articular surface. This permits control over both parts and the reduction of the articular surface. Due to the design of anatomic shaped locking plates, the locking of the articular segment of the plate is possible through that approach. The locking of the shaft component of the plate can be achieved through stab incisions. This surgical method was mainly used for articular fractures in this study. In some articular fractures, an additional incision was made to gain better control of the fractured articular surfaces (Fig. 5). However, it can be summarized, that 2 distinct small approaches which are placed rather deliberately, provide better fracture control than a single long one. Therefore, the soft tissue does not need to be pulled and torn.
Fig. 5
Clinical presentation of a distal femur fracture following the implementation of two distinct incisions directly over the fracture site (white arrow) and the joint (black arrow)
Most non-articular fractures required a direct approach onto the fracture and percutaneous locking of the plate proximal and distal to the fracture (Fig. 6). This permitted direct fracture control and facilitated reduction (21 out of 24 non-articular fractures).
Fig. 6
a: Clinical depiction of minimally invasive incisions (3.5 cm) and stab incisions executed in the scenario of a forearm fracture (AO: 2R2A3, 2U2A3). b: Postoperative radiographic imaging captured in two dimensions, showcasing plate osteosynthesis and fracture realignment
If fracture reduction was attained through closed methods or percutaneously, the plate was positioned eccentrically, as depicted in Fig. 4. This approach to fracture reduction was employed in only 3 cases out of the 24 non-articular fractures.
The difference between these 2 methods is best described for clavicular fractures. While the most common surgical technique is a double incision without direct control of the fracture, by applying MIO approaches, a small incision is placed slightly lateral to the fracture for reduction and lateral locking, hence locking the plate medially-percutaneously [15, 34].
In our opinion, fracture control is essential for articular- and non-articular fractures. Contrary to that, most published techniques for MIO in non-articular fractures describe to direct fracture contract. Fluoroscopically controlled reduction is timely and technically inferior to open reduction and a small approach placed on a crucial landmark often suffices to optimize fracture reduction. In shaft fractures with a large fracture zone, the key landmark for reduction should be identified and the incision placed right above it.
Mainly standard approaches were used for the location of MIO surgical approaches. It permitted a fallback option for complex fractures in case reduction itself was not able to be sufficiently carried out. In such cases, an extension of the approach would permit for maximal fracture control.
Hence, in articular fractures the main incision was placed to control the articular surface and the fracture. In non-articular fractures, the incision was placed directly onto the fracture.
Closed reduction was used by applying traction and counter traction during surgery as well as adequate patient positioning on the operating table. Many techniques were combined, depending on the type of fracture to achieve an adequate reduction. For the same anatomical regions, similar techniques were used. It can be summarized that a sufficient MIO technique requires a precise planning based on imaging, the percutaneous application of reduction tools, K-wires and reduction clamps. In extensive approaches, reduction tools were usually applied directly to the bone through the main approach. This MIO reduction technique my require some training and a learning curve, especially to avoid soft tissue damage by crushing reduction clamps due to mispositioned percutaneous incisions [35]. Further, in regions with delicate anatomic structures, a thorough knowledge of their anatomic position is required to avoid accidental damage. In distal humeral fractures where the ulnar nerve is exposed in open techniques, special attention must be taken for its protection [23].
In 29 cases, a plate was used as a reduction aid itself (Fig. 7). This technique seems to be specific for MIO. Compared to classical surgical sequences, in MIO the reduction and fixation can be executed simultaneously by using the plate.
Fig. 7
a: Intraoperative anterior-posterior radiograph of a multifragmentary proximal humerus fracture. b: Application of the stable-angle plate osteosynthesis and elevation of the dislocated humeral head with the raspatory. c: Fixation of the plate in the area of the humeral head and shaft with Kirschner wires and reduction of the axis by a cortical screw over the plate (white arrows). d: Final radiographic control with double plate osteosynthesis in two planes
In proximal humerus fractures for instance, this technique proved to be efficient, especially when using multiple drill sleeves. Tightening a plate dependent lag screw through the plate that is temporarily fixed to the bone using K-wires, reduces the greater tuberosity to the shaft and restores valgus malalignment or medial dislocation of the shaft. In tibial head fractures, the compression of the head can be applied safely using the anterolateral plate as a pressure converter, similar to washers or plates on the medial side of the tibial head. The lateral wall of the tibial head will then be realigned. An anatomic plate tightened onto the bone will reduce partially some dimensions of fracture dislocation. Applied from one side in long bones, it will reduce side-to-side and varus/valgus malalignment. Further, when the plate is centered to the bone, the ante/recurvation is corrected.
However, it can be assumed that closed reduction techniques are practically more challenging than open ones. This difference will become even more relevant for complex and comminuted fractures in anatomic regions where an anatomic reduction is necessary.
The identification of key landmarks seems important for estimating the possible reduction. The control of these landmarks permits a successful reduction. The palmar cortex for distal radius fractures or the anterior and posterior fracture borders of the fibula in malleolar fractures are such landmarks. Minimal invasive approaches for these landmarks suffice for fracture reduction and a plate can be slid in. This includes distal radius fractures, where 1,5 cm approaches were described [22]. In such cases, the locking and positioning of the plates might be more difficult than the reduction itself.
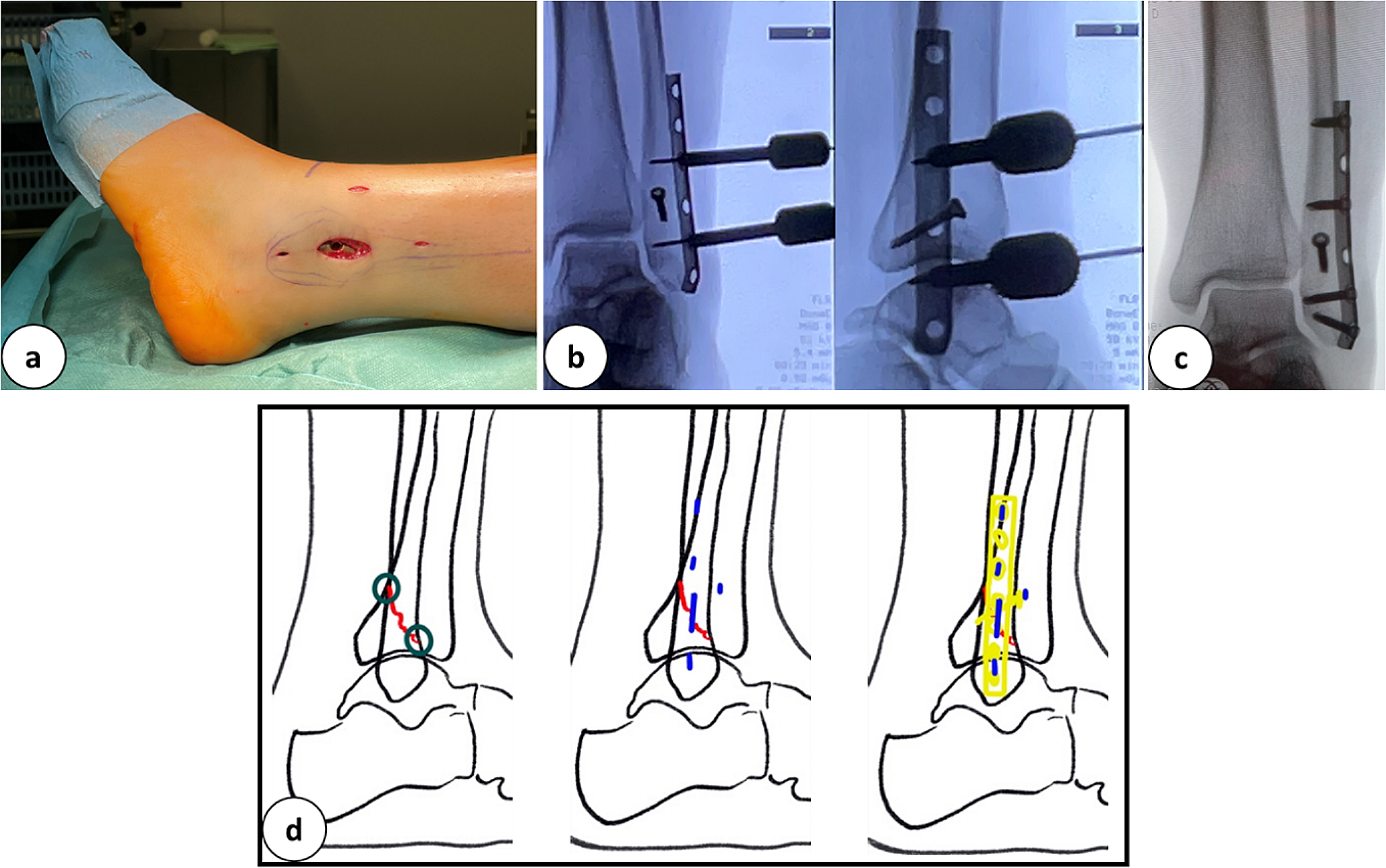
The condition of soft tissues is crucial to decide upon fracture treatment with MIO. In some severe open fractures with a foreseen primary delay of wound closure, an alternative and less invasive approach might reduce secondary damage to soft tissues and decrease the risk for infection (Fig. 8).
Fig. 8
a: Anterior-posterior X-ray and 3-D computed tomography scan of a tibial plateau fracture (AO: 33C3.3). b: Preoperative clinical images before minimally invasive double plate osteosynthesis with a knee joint bridging external fixator. A condition after compartment release. c: Clinical images after minimally invasive double plate osteosynthesis and wound closure. d: Intraoperative final X-ray in 2 planes with double plate osteosynthesis. e: X-ray control 10 days postoperatively with double plate osteosynthesis in the area of the tibial head and miniplate with screw osteosynthesis of the patella
In osteoporotic fractures (Fig. 9) with closed but damaged soft tissues, MIO might be a safer alternative, even when an anatomic reduction is not possible. In these cases, complex reconstruction methods for bone and soft tissues should be avoided, as their failure risk is high due to the patients age, anticoagulation, and comorbidities, such as diabetes, vascular diseases, and polyneuropathy. In some obese patients, a MIO might not be achievable at all.
Fig. 9
a: Anterior and lateral slices of a computed tomography scan of a multifragmentary distal tibial fracture with a pilon fracture. b: Lateral intraoperative radiographs before and after reduction of the distal tibial articular surface. c: Clinical images of the surgical approaches postoperatively before wound closure. d: Intraoperative final radiographic control after plate osteosynthesis and set screw implantation in 2 planes. e: Radiograph in 2 planes after removal of the set screw and fracture consolidation, 12 weeks postoperatively
It can be summarized that combined reduction techniques, percutaneous and open lead to satisfactory fracture reduction results. The plate itself plays a crucial role in the reduction technique itself [28].
The insertion of the plate is especially interesting because it used to be the determinant factor for the length of the approach. Percutaneous screw insertion and locking of the plate has become practicable through the use of drill sleeves. It permits drilling, measuring using the drill bit, and the insertion of the locking screws through stab incisions. The LISS guiding arm was one of the first implants, apart from nails, to promote this locking through stab incisions. Nevertheless, locking through stab incision is feasible with drill sleeves only without using a guiding arm. Hence, it can be concluded that the length of the approach should only be planned for reduction. In articular fractures, this can usually be implemented and plate approaches for plate insertion are mainly needed in non-articular fractures. Only 8 out of 57 fractures required a plate approach, and 7 were non-articular fractures (n = 24). Out of 33 articular fractures, only 1 needed a plate approach. The goal for plate insertion should be to use the existing approach for fracture reduction.
Hence, plate locking doesn’t need direct incisions other than various stab incisions.
LimitationsNotable technical differences to non-MIOs were the percutaneous application of clamps (n = 9) and K-wires (n = 15). The application of pointed reduction clamps needed additional stab incisions for the clamp tine, and K-wire insertion required planning to avoid damage to structures at risk. Although not evaluated, adequate plate positioning is more cumbersome in MIO than in ORIF and usually needs to be verified fluoroscopically.
Other disadvantages, such as increased surgical duration and radiation exposure were widely discussed in the literature, and some benefits outweigh them. A further limitation of this study is its retrospective setup.
留言 (0)