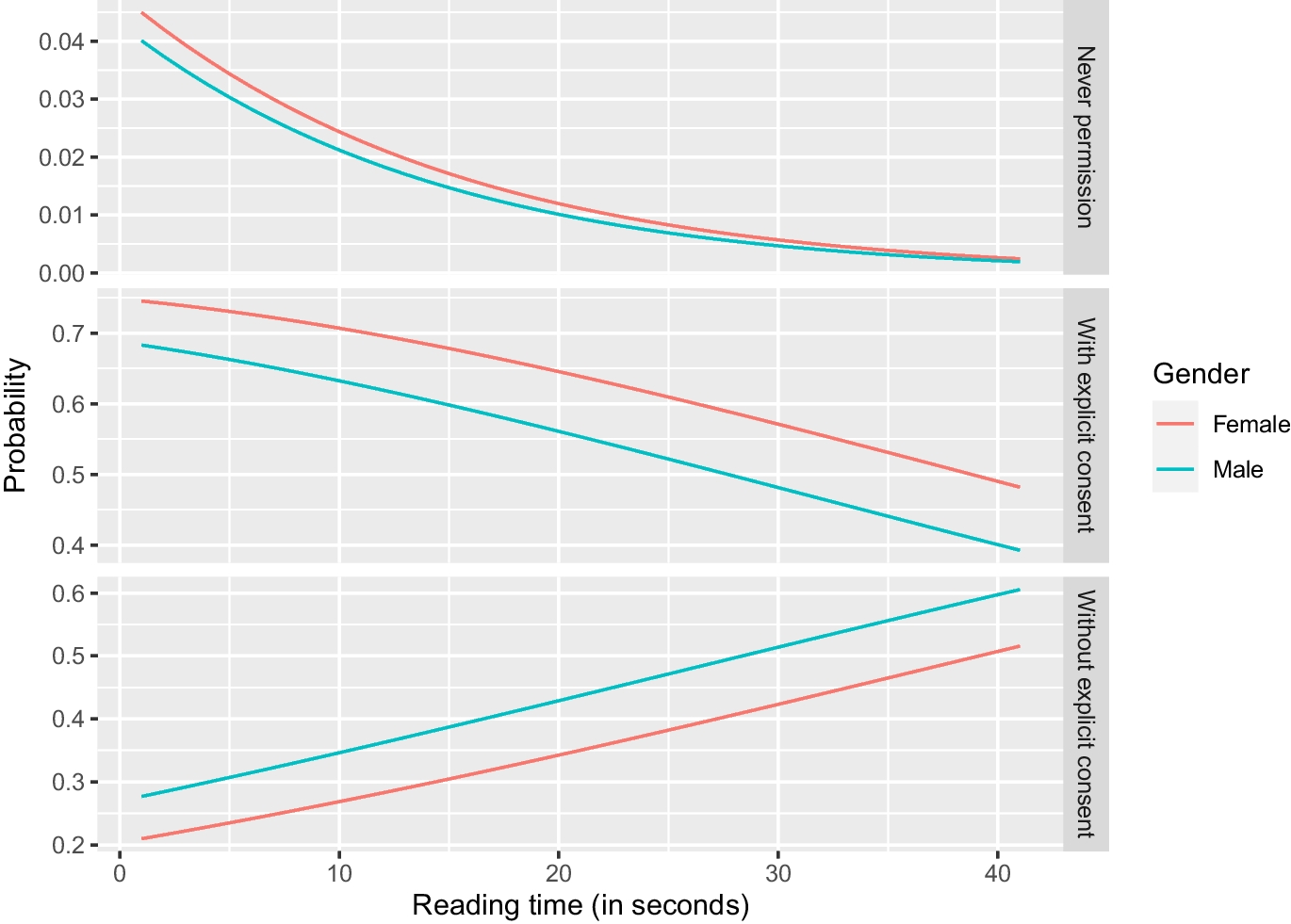
The results of this study show that the view of the general population on the retrospective use of diagnostic imaging data for research purposes is variable, depending on the setting. Although the vast majority would allow hospitals to perform retrospective research with diagnostic imaging data (97.4 per cent), this proportion drops somewhat for universities (89.7 per cent), other non-commercial institutions (82.4 per cent), and government agencies (79.5 per cent), while only a minority would allow commercial firms to use their diagnostic imaging data (36.5 per cent). This finding may be explained by the fact that patients already have a relationship with their hospital based on some degree of trust and that this trust decreases in institutions with which such a relationship did not exist. It also shows that government agencies are not completely trusted, especially by respondents with primary education as highest level of education completed, and that faith in for-profit companies is generally lacking. Another finding of this study is that the majority of participants indicated their explicit consent to be required before any diagnostic imaging data can be used for retrospective research. Importantly, however, whether or not participants deemed consent necessary depended on two variables, namely the time spent on reading the explanation about retrospective radiology research in this survey and level of education. Participants who spent more time on reading the explanation about retrospective radiology research more frequently indicated no need for their approval to execute such studies. In fact, when including only those participants (32.0 per cent) who spent at least the minimum reading time to be able to comprehend the text (12.3 s), the preference for a waiver of consent increased by ten percentage points, to 41.0 per cent. This is also in line with the finding that a majority of patients do not read informed consent texts (Özhan et al. 2014). The variance in time spent on reading the explanation about retrospective radiology research can be explained by the fact that the participants previously answered several other questions related to radiology in this survey (that were not part of the present study) and that some participants may have been impatient or considered it unnecessary to read the full explanation. Younger respondents and respondents with a lower level of education were less likely to take (sufficient) time for reading the text than older and higher educated respondents. People who had completed a higher level of education also more frequently indicated informed consent to be unnecessary compared to lower educated people. This is in line with a large body of previous literature that has suggested that education leads to higher trust (cited in Wu 2021), where the Netherlands is in the top ten countries with a positive correlation, ranking close to smaller countries like Slovenia and Trinidad and Tobago, but also larger countries like the United States. Finally, it should be noted that participants’ view on the retrospective use of diagnostic radiology data was similar to their view on the retrospective use of interventional radiology data.
Our findings may have two potential practical implications. First, policymakers may perhaps be more lenient towards permitting the use of deidentified radiology data without requiring patient informed consent, provided the situation concerns a hospital setting and patients are well informed about what retrospective radiology research entails (in this situation, a substantial proportion of respondents indicated explicit patient consent to be unnecessary). This approach is not in line with the GDPR article 5, where it is stated that data that is “collected for specified, explicit and legitimate purposes and not further processed in a manner that is incompatible with those purposes” (European Commission 2022). However, studies have shown that, under certain conditions, people are nevertheless willing to share data for health research (Kalkman et al. 2022), and they are also less likely to revoke once having given consent (Kreuter et al. 2020). Therefore, patients may be assumed to have no objections to having their imaging data being retrospectively investigated unless indicated by an opt-out option that should be readily available to patients and visible to researchers. However, the passive nature of opt-out causes an opt-in procedure a preferred standard (Lutomski and Manders 2024). Moreover, opt-out procedures may increase administrative burden (Marcotte et al. 2023). In addition, for patients to be able to make a well-informed decision to make use of this opt-out option, hospitals or radiology departments may be encouraged to enclose additional information on this topic in patient brochures and/or pamphlets, and by verbal communication to those who undergo medical imaging. This information should be adapted to those with lower levels of education, as our research has shown lower educated people to be generally more reluctant towards letting researchers retrospectively investigate their imaging data. Especially interactive components in the informed consent process to facilitate understanding are important (Glaser et al. 2020). Second, for all other institutions that do not concern a hospital (i.e. universities not linked to a hospital, other non-commercial institutions, government agencies, and particularly commercial firms), the support for an informed consent waiver for retrospective radiology research drops dramatically, and for these institutions, it can be argued that an “opt-out option” would be inappropriate, and that all patients should be actively approached and asked for informed consent to use their imaging data.
This present study had some limitations. First, our study was performed among participants who can be considered representative of the Dutch population, and it remains unknown if our findings are also applicable to other countries. Second, our study did not investigate the general population’s view on more complex issues such as situations in which non-commercial investigators work together with commercial partners and when researchers aim to investigate imaging data linked to genetic data. Third, for the sake of not introducing too much complexity, we did not specifically inform participants about the difference between fully anonymized and pseudonymized data. Fourth, we speculated about potential practical implications of our findings (i.e., assumption of no patient objection for retrospective radiology research by hospitals unless indicated by patients and assumption of patient objection for retrospective radiology research by all other institutions unless explicitly permitted by patients), but whether or not the population would actually accept these scenarios remains unclear. Furthermore, it should also be emphasized that previous research on this topic has been completely lacking so far. Therefore, the results of our study should be considered as a baseline measurement of the general population’s view on retrospective radiology research and to serve as a basis for further studies.
In conclusion, the general population permits retrospective radiology research by hospitals, and a substantial proportion indicates explicit patient consent to be unnecessary when understanding what retrospective radiology research entails. However, the general population’s support for the unrestricted retrospective use of imaging data for research purposes without patient consent decreases for universities not linked to hospitals, other non-commercial institutions, government agencies, and particularly commercial firms.





留言 (0)