This quantitative study is to our knowledge the first to investigate the prevalence and experience of UI among elite female Gaelic sports athletes (Camogie and Ladies Gaelic Football players) in Ireland. The differences between the Camogie and Ladies Gaelic Football players regarding age, BMI, parity, presence of medical risk factors, and total fluid intake were relatively small and considered to be of no clinical significance. Camogie players were found to have a higher consumption of weekly units of alcohol and the Ladies Gaelic Football players were found to have a higher consumption of bladder-irritant fluids and interestingly, the Ladies Gaelic Football players reported significantly longer weekly sporting activity time (p = 0.04), which was identified as a significant risk factor for UI in this current study.
Prevalence of UI
Although the prevalence of UI was slightly higher among the Ladies Gaelic Football players than among the Camogie players, there was no significant difference between sports in the prevalence of UI, the prevalence of SUI, UUI, MUI, or the EDL or ICIQ-UI-SF scores.
The overall prevalence of UI among these elite players was high (61.6%). This may not be surprising owing to the high velocity, high impact, and physical nature of the two sports, which include kicking a large ball (Ladies Gaelic Football) or striking a sliotar (Camogie), as well as running, sprinting, jumping, catching, and passing over a large 145 m × 90 m pitch. Research has indicated that high-impact sports, elite status, and long hours of training are risk factors for UI [3, 6, 7, 25], which is supported by the findings of the current study, with logistic regression indicating that players who had longer weekly sporting activity time were significantly more likely to experience UI.
Rugby is a high-impact team sport played on a large grass pitch and a study by Sandwith and Robert involving Canadian Intervarsity female rugby players found that over half (54%) reported UI [20]. A recent study by McCarthy-Ryan et al. investigating the prevalence of UI among female rugby players in the UK and Ireland, who were playing rugby at any level, reported a rugby-related prevalence of SUI of 43% [26]. Pires et al., in a review evaluating the prevalence of UI and the influence of sport modality, reported that the prevalence of UI in high-impact sports (involving running and jumping) ranged from 14.3% to 75.6%. Of the team sports, volleyball (75.6%) was found to have the highest prevalence, followed by indoor football (50.0%) [8]. Gaelic sports involve less jumping than volleyball, but more jumping than rugby and indoor football, and this could potentially explain the relative prevalence of UI reported here.
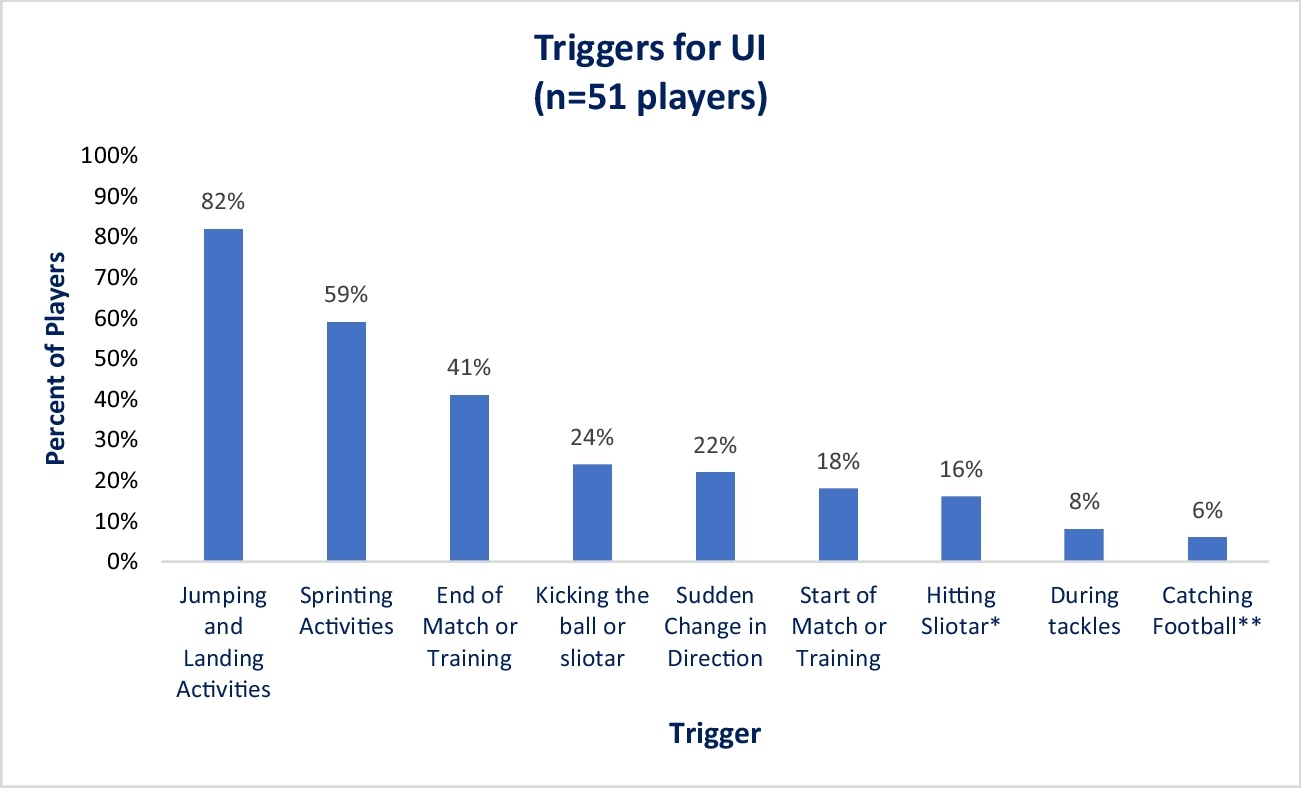
Stress urinary incontinence (52.0%) was the most common form of UI reported in this study, and almost one-third reported MUI, with few (7.1%) reporting UUI only. Of those players who reported triggers for their UI, over four-fifths (42 out of 51) reported jumping activities and over half (30 out of 51) reported sprinting activities to be triggers. This is consistent with the findings of previous research reporting that SUI is the most common form of UI among high-impact athletes and is considered to be a consequence of the increased abdominal pressure experienced and the impact of ground reaction forces on the pelvic floor during high-impact sport [6, 8, 25]. In addition, around two-fifths of the players reporting triggers said that UI occurred toward the end of matches or training, potentially suggesting pelvic floor fatigue [21].
Although not found to be statistically significant in the regression analysis model, the results suggested that players who included more bladder irritants in their fluid intake were more likely to experience UI, which corresponds with findings from previous research literature [16, 17]. This suggests a need for education regarding bladder health and type of fluids among the players.
Parity appeared to influence the prevalence of UI, with all eight parous players experiencing UI. Four parous players sought treatment, although it is unknown if these players sought treatment before or after returning to their sport. Groom et al. recently published a return to running after pregnancy protocol that highlighted the fact that postpartum women benefit from individualized pelvic floor assessment and rehabilitation for the prevention and management of PFD on their return [27]. A recent qualitative study by Davenport et al. suggested that there appears to be limited support for elite female athletes in their return to sport postpartum and that there is a need for evidence-based return-to-sport protocols [28]. Interestingly, half of the parous players did not receive treatment for their UI. Future research should include surveying or interviewing past county players to explore if PFD and UI post-childbirth was a factor in leaving elite-level play and if they were aware of the treatment options available. Consideration should be given to the development of a protocol for a return to Gaelic sport postpartum following further mixed-methods research conducted with these elite players.
Knowledge of PFMs/PFMT and Experience of UI (Impact, Triggers, Strategies, and Treatment)
Although many players knew where the PFMs are, and 41% had learned about PFMT, not all were confident in performing the exercises and few players had done PFMT within the last 4 weeks. UI is a treatable condition. However, only 10 players reported receiving treatment for their UI, and this was most commonly from a physiotherapist and mainly in the form of PFMT. A Cochrane review found that PFMT can improve or cure UI and is most effective in the treatment of SUI [29]. Similar to the findings of previous research, these data suggest a need for education around PFMT and treatment in these elite players [3, 6,7,8,9]. In addition, future research should consider evaluating the effect of PFMT in elite Gaelic sports athletes.
The mean (SD) ICIQ-UI-SF severity score of 6.13 (3.37) was within the moderate range (6 to 12 out of 21) [30]. Despite the high prevalence and moderate severity, the impact of UI on the players’ everyday life was relatively low (mean (SD) EDL score/10 of 2.29 (2.28)), which may be expected in a predominantly nulliparous group of relatively young players.
Few players spoke to another person about their UI and most commonly spoke to family or friends. Although few discussed their UI or sought help for what is a treatable condition, many players reported using strategies to try to manage and mitigate their symptoms. The strategies most commonly used were pre-voiding, wearing protection, modifying or changing clothing during sports, or reducing fluids, the latter of which is of concern owing to the need for appropriate hydration in athletes. Once again, this suggests a need for education regarding UI/PFD and treatment options available and is consistent with the findings of previous research [6, 7, 9].
Strengths and Limitations
The strengths of this study include the fact that the sports included have not been investigated to date and, although the questions exploring players’ experiences were quantitative in nature, the responses helped to inform the interview guide for the qualitative component of the larger mixed-methods study. Limitations include the relatively low response rate from the overall number of Gaelic players. It is also acknowledged that players who were experiencing UI may have been more likely to respond than players who were continent. Therefore, findings regarding the prevalence of UI and associated risk factors must be interpreted with caution and viewed as prevalence amongst this cohort of female players. However, having a total of 185 responses from these elite female athletes who were playing two different sports adds to the international literature about sportswomen’s experience of UI and new knowledge in Ireland. In addition, the prevalence reported here is similar to that of other high-impact, field-based sports played on a large grass pitch, such as rugby [20].
This study involved female Gaelic sports athletes who were 18 years and older, predominantly nulliparous, playing at an elite level, with long hours of training, and therefore the results may not be generalizable to club-level Camogie and Ladies Gaelic Football players, or to other sports. Further research into the prevalence and experience of UI could include club-level and adolescent female Gaelic sports players.


留言 (0)