
記住我


A total of 328 patients were identified and included in the analysis. The characteristics of these patients are summarized in Table 1. Patients were a median of 63 years (range, 29–85) old at time of WBRT. The proportion of male and female patients was 44% (n = 145) and 56% (n = 183), respectively. The most common primary tumor histology was NSCLC (41%), followed by breast cancer (22%), small cell lung cancer (SCLC; 13%) and melanoma (9%). Less common primary tumors (all with ≤ 10 cases included) were prostate (3%), esophageal and gastric (2%), gynecological (2%), colorectal (1%), head and neck (1%), and other including undifferentiated histologies (5%). In patients with NSCLC, targetable mutations in the epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) genes were known to be present in 8% and 4% of cases, respectively. In patients with breast cancer, human epidermal growth factor receptor 2 (HER2) mutations were present in 27% of cases, whereas 22% had triple-negative disease.
Table 1 Characteristics of patients who underwent WBRT for brain metastasesThe initial treatment intent, at time of first cancer diagnosis, was curative in 145 patients (44%), and palliative in 183 patients (56%). The median KPS at time of WBRT was 80 (range, 30–100), and extracranial disease was present in 80% of patients. Most patients had ≥ 10 brain metastases (n = 172; 52%), with the remaining patients having either 4–9 (n = 77; 23%) or ≤ 3 metastases (n = 79; 24%). Evidence of leptomeningeal disease (with or without parenchymal metastases) was present in 56 patients (17%).
The most common WBRT dose-fractionation scheme was 30 Gy in 10 fractions (n = 210; 64%), followed by 20 Gy in 5 fractions (n = 82; 25%), and 24 Gy in 6 fractions (n = 12; 4%). The remaining 24 patients (7%) were treated with individual dose-fractionation schemes (total dose 18–46 Gy in 4–23 fractions). A focal boost to macroscopic disease was delivered in 37 patients (11%). Patients treated in ≥ 10 fractions had a better KPS than those treated in < 10 fractions (p < 0.01), although age was not different between these groups (p = 0.21). WBRT was completed as scheduled by 302 (92%) patients. In the remaining 26 patients (8%), WBRT was stopped early due to clinical deterioration or patient choice.
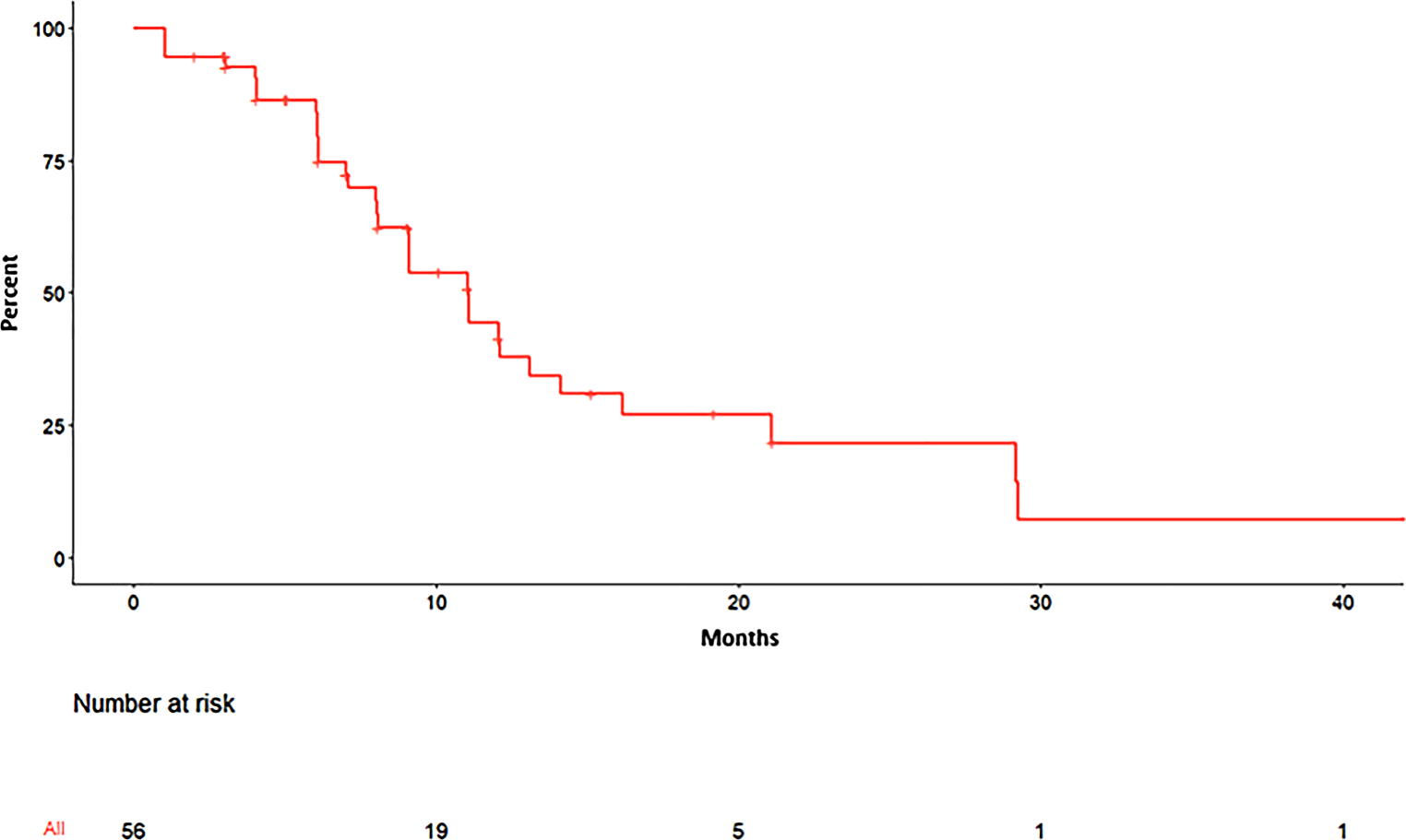
Median follow-up was 4.4 months (range, 0.1–154.3 months). The KM estimates of survival are shown in Fig. 1. Median OS for the entire cohort was 4.7 months (95%CI, 3.8–6.0) after WBRT. OS differed between primary tumor type (p < 0.01; Fig. 1a), with the longest survival seen in patients with breast cancer (median 7.7 months; 95%CI, 5.1–10.2). In comparison, patients undergoing WBRT for metastases of NSCLC (the largest subgroup) had a median OS of 4.8 months (95%CI, 3.2–6.1). Patients with SCLC and melanoma had a median OS of 3.5 months (95%CI, 2.1–6.4) and 4.6 months (95%CI, 2.0–9.2), respectively, whereas patients with other histologies had a median OS of 3.0 months (95%CI, 1.7–4.9). OS also differed between patients stratified by KPS (p < 0.01; Fig. 1b). Patients with a KPS of 90–100 survived for a median of 8.3 months (95%CI, 7.0–13.0), compared to 4.1 months (95%CI, 3.5–6.1) in patients with KPS 70–80, and 1.7 months (95%CI, 1.2–2.6) in patients with KPS < 70 (p < 0.01).
Fig. 1
Kaplan-Meier estimates of overall survival following WBRT for brain metastases, stratified by primary tumor type (left panel) and KPS (right panel). More favorable survival outcomes were observed in patients with breast cancer, as well as in those with a good performance status. Abbreviations: KPS Karnofsky Performance Status, NSCLC non-small cell lung cancer, SCLC small cell lung cancer, WBRT whole brain radiation therapy
Results of the multivariate Cox regression analysis are shown in Fig. 2. Neither the patients’ sex nor age group were significant covariates for death after WBRT in our cohort. The covariate with the largest effect size was KPS, with a HR of 0.50 and 0.35 for patients with KPS 70–80 and 90–100, respectively (p < 0.001). The lowest HR of death was seen in patients with breast cancer (HR 1.0; reference), whereas patients with metastases from melanoma (HR 2.01; p = 0.007) and SCLC (HR 2.12; p = 0.002) appeared to have the worst outcomes. The presence of extracranial metastases (HR 1.48; p = 0.016) and leptomeningeal disease (HR 1.58; p = 0.012) was detrimental, whereas primary tumor control was not a significant factor (HR 0.95; p = 0.738) in the model. In patients who completed WBRT as scheduled (n = 302), those who received a dose of ≥ 30 Gy had a significantly lower HR of death (HR 0.45; p < 0.001) than those who had received < 30 Gy. Delivery of a boost to macroscopic disease was not associated with a lower HR of death, although a statistical trend could be observed (HR 0.70; p = 0.089).
Fig. 2
Multivariate Cox regression analysis showing the HR of death after WBRT in patients with brain metastases. Abbreviations: HR hazard ratio, KPS Karnofsky Performance Status, NSCLC non-small cell lung cancer, SCLC small cell lung cancer, WBRT whole brain radiation therapy
Patients were reclassified according to the Rades scoring system, as described previously [20]. The KM estimates of OS for these different subgroups are shown in Fig. 3. Survival outcomes differed between subgroups based on the Rades scoring system (p < 0.01): median OS was 1.9 months (95%CI, 1.4–3.6), 2.7 months (95%CI, 2.2–3.6), 6.1 months (95%CI, 4.8–7.6) and 14.5 months (95%CI, 6.4–44.0) for groups A–D, respectively. The 6‑month survival rates for groups A–D were 17% (95%CI, 8–35%), 31% (95%CI, 22–44%), 50% (95%CI, 44–58%) and 66% (95%CI, 50–85%). For reference, the 6‑month survival rates in the original Rades cohort were 6%, 15%, 43% and 76% for groups A–D, respectively [20].
Fig. 3
OS in patients classified according to the Rades scoring system, which was previously developed for patients undergoing WBRT for brain metastases. Survival outcomes differed between Rades subgroups in this more contemporary cohort, with a stepwise increase in OS seen from group A (poorest outcome) to D (best outcome). Abbreviations: OS overall survival, WBRT whole brain radiation therapy
留言 (0)