
記住我

Bispecific antibodies [bsAb] targeting B-cell maturation antigen [BCMA] and G-protein-coupled receptor class C group 5 member D [GPRC5D] have demonstrated deep and durable responses in patients with relapsed/refractory multiple myeloma [MM], with single-agent response rates from 57–71% [1,2,3,4,5,6]. Currently, two BCMA- and one GPRC5D-targeting bsAb—teclistamab, elranatamab, and talquetamab, respectively—have received FDA accelerated approval in patients with relapsed/refractory MM after four or more prior lines of therapy. Notably, in their pivotal trials, the bsAb was administered continuously until disease progression or intolerance. However, fixed-duration dosing with treatment-free interval(s) is being explored [7, 8] and maybe a preferred approach from both efficacy and safety standpoints for several reasons. First, continuous exposure to T-cell engaging bsAb can lead to T-cell exhaustion, as highlighted in preclinical studies, and treatment-free intervals are associated with transcriptional reprogramming and functional reinvigoration of T-cells [9]. T-cell exhaustion from continuous dosing may lead to lower efficacy of subsequent T-cell redirecting therapies, as potentially suggested by lower response rates to cilta-cel among patients with prior bsAb exposure [10]. Second, continuous exposure may drive some mechanisms of relapse. Correlative studies on plasma cells at relapse have shown a higher incidence of mutational events or biallelic loss affecting the BCMA-encoding gene TNFRSF17 following bsAb than after CAR T-cells (43% vs 6%, respectively) [11]. Third, infection-related morbidity and mortality have emerged as one of the key toxicities with BCMA bsAb in MM [12,13,14], with the depth and duration of immunosuppression likely to correlate strongly with the duration of bsAb exposure. In the MajesTEC-1 trial, patients who switched to bi-weekly dosing of teclistamab after 1 year had a substantially lower incidence of grade ≥ 3 infections compared to those who remained on weekly dosing (16% vs 33%, respectively) [15]. Finally, fixed-duration treatment would lower therapeutic burden and time-toxicity for patients, and reduce financial impact on payers and healthcare systems, improving accessibility globally.
Although there are no prospective data on the response durability with fixed-duration dosing of BCMA or GPRC5D bsAb in MM, several patients in bsAb trials discontinued treatment for reasons other than disease progression. We performed a multi-institutional retrospective cohort study to investigate the outcomes of patients enrolled in early-phase BCMA- or GPRC5D-bsAb trials or receiving standard-of-care bsAb at six academic medical centers, who discontinued bsAb for reasons other than disease progression or death, with at least 3 months’ remission after drug discontinuation. This study was approved by the institutional review boards at each participating center.
Among 201 patients receiving BCMA or GPRC5D bsAb as single agent, 23 patients met the inclusion criteria and were thus included in our study. Median age was 68 years [range, 28–92], with 52% female, and 7/23 [30.4%] belonging to racial/ethnic minorities [including Black, Hispanic, or Asian as per self-reported data from electronic medical records]. High-risk cytogenetic abnormalities [HRCA] by FISH were present in 10/23 patients, with the most common being gain(1q) [n = 8], followed by del(17p) [n = 3], t(4;14) [n = 1], and del(1p) [n = 1]; ≥ 2 HRCAs were present in two patients. Patients had received a median of four lines of therapy prior to bsAb [range, 3–9], including 17 patients with prior autologous transplants (six of whom had had two prior autografts) and two patients with prior allogeneic transplants. BsAb target was BCMA in 20 and GPRC5D in three patients. All but one patient had achieved a very good partial response [VGPR] or better to bsAb prior to treatment discontinuation, including 16 patients with CR/sCR, 6 with VGPR, and 1 PR. Median time to best response was 3.1 months [range, 0.23–8.5]. Median duration of bsAb treatment prior to discontinuation was 7.6 months (range, 1–52). The most common cause for treatment discontinuation was infection [n = 12], followed by second malignancy [n = 2], neutropenia [n = 2], failure to thrive [n = 2], non-adherence [n = 1], onset of COVID-19 pandemic [n = 1], severe fatigue [n = 1], neuropathy [n = 1], and sponsor decision to terminate the trial [n = 1].
At a median follow-up of 15.5 months from bsAb discontinuation (range, 3–32.3), 19/23 patients [82.6%] are alive and progression-free, with estimated Progression-Free Survival (PFS) at 6, 12, and 18 months of 90.5% (95% CI, 78.8–100), 84.0% (95% CI, 68.7–100), and 70.0% (95% CI, 46.4–100), respectively. The Kaplan–Meier curve for PFS is shown in Fig. 1. A swimmer plot showing the trajectory of all 23 patients is shown in Fig. 2, and clinical/demographic characteristics of the included patients are highlighted in Supplementary Appendix I. Notably, the sole patient in PR remained in remission at data cut-off, however, had only 3 months of follow-up after discontinuation. All four patients with relapse had sCR as their best response to BCMA bsAb, and their disease relapsed at a median of 7.3 months [range, 3.6–18] after bsAb discontinuation. The three patients who had received GPRC5D-targeting bsAb remain in remission at the time of writing, at 10, 11, and 25.5 months from treatment discontinuation, respectively. Notably, 2/4 patients whose disease relapsed had high-risk cytogenetics by FISH at baseline [gain(1q), and triple-hit with t(4;14), del(17p), and gain(1q), respectively]. Treatment received after relapse and associated responses were as follows (one patient each): talquetamab (achieved sCR); cyclophosphamide-bortezomib-dexamethasone (no response); elotuzumab-pomalidomide-dexamethasone (no response); and none, due to non-adherence. Among patients with a sustained response, all maintained or improved their response depth at latest follow-up. No deaths have been reported thus far since bsAb discontinuation.
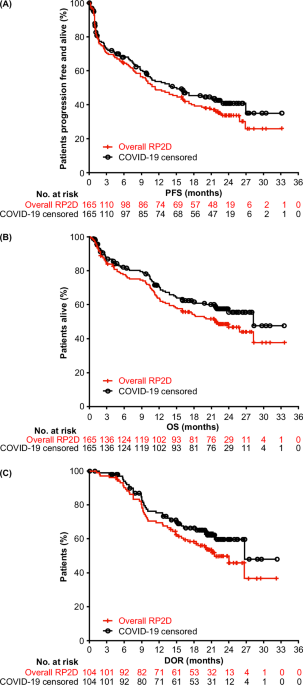
Fig. 1
Kaplan–Meier curve for progression-free survival from discontinuation of bispecific antibody in patients with relapsed/refractory myeloma.
Fig. 2
Swimmer plot for outcomes in all 23 patients who discontinued bispecific antibodies for a reason other than progression or death and had at least 3 months of follow-up after drug discontinuation, commencing at the time of discontinuation.
We demonstrate that for patients with heavily pre-treated relapsed/refractory MM who stop bsAb due to reasons other than progression or death, over 80% remained in a sustained remission at 1 year. In relapsed/refractory MM, the FcRH5xCD3 bsAb cevostamab has been studied as a fixed-duration therapy for ~1 year [7]. Among 16 patients in the phase 1 trial that completed therapy, 13 [81.3%] remained in remission at latest data cut-off, with 8 sustaining their response ≥ 6 months and 3 sustaining response ≥ 12 months after treatment completion [7]. In that trial, 3 patients had progressed thus far [1 from PR and 2 from VGPR] at 1.3, 7.8, and 12.9 months from treatment initiation, respectively. Analogously, in relapsed/refractory diffuse large B-cell lymphoma, a fixed-duration (12 cycles) of CD20xCD3 bsAb, glofitamab, led to durable CRs (median duration of CR, 34 months) [16]. Among 35 patients who achieved CR, just 4 patients had relapsed or died at latest follow-up. In follicular lymphoma, CD20xCD3 bsAb mosunetuzumab uses a response-adapted, fixed-duration approach [17]. In MM, in addition to cevostamab, the GPRC5D bsAb forimtamig is also being studied in a fixed-duration regimen for 1 year in relapsed/refractory MM [NCT04557150]. Another phase 2 single-arm study [LimiTEC, NCT05932680] is testing monitored drug discontinuation after 6–9 months of single-agent teclistamab among patients who achieve ≥ VGPR, with the primary endpoint being failure-free survival at 6 months after discontinuation [8].
Our findings of sustained remissions in bsAb-responding patients who stop treatment for reasons other than progression add to the growing evidence base [9, 11, 13] that highlights the urgent need to test fixed-duration bsAb approaches. These data support prospective trials exploring fixed-duration, response-adapted, and/or extended pauses of bsAb therapy since tumor cell clearance can occur very early with bsAb. A consistent and nuanced definition of the target population will be important to inform results, especially given the heterogeneity of evolving tumor phenotypes [18]. Although the majority of patients in our study remained in remission for over 6 months off treatment, there was heterogeneity regarding the duration of remission/follow-up. Additionally, MRD status at treatment discontinuation and longitudinal MRD testing were not routinely performed. Since an overwhelming majority of our patients (20/23) were in CR/sCR at the time of treatment discontinuation, the data may not be applicable to patients with less than a VGPR. Future studies should assess clinically actionable biomarkers of tumor and immune microenvironment, including longitudinal MRD assessment, to identify individuals who are at higher risk of relapse following treatment discontinuation [19]. Although re-exposure to the same bsAb treatment at re-emergence of disease was not tested in this cohort, future trials should prospectively test re-treatment, potentially in combination with monitoring for escape mechanisms such as antigen loss [11].
留言 (0)