This study observed a significant increase of 39.0% (p < 0.001) in TSCI’s in admitted patients with spinal fractures over the past 35 years (Fig. 2b). The increase in spinal fractures in admitted patients in total was not statistically significant (p = 0.466, Table 1). In thoracic and lumbosacral spinal fractures, the incidence in TSCI seems to have decreased since 1986, which was not the case for cervical fractures as it showed a 132.2% increase.
We saw an increase of 84.9% in patients presenting with spinal fractures to the ED since 1997 in the Netherlands, which is in line with current literature(Fig. 3) [1, 26]. Multiple explanations for this increase in overall spinal fractures can be given. Most notably, the increase in computed tomography (CT)-scan usage resulted in higher detection rate [27, 28]. Also, the Dutch population is aging, meaning an increasing amount of osteopenia and osteoporosis throughout the population [1]. Smits et al. found a much faster increasing incidence in spinal fractures in the elderly compared to the younger population in The Netherlands [26].
The increase in TSCI in admitted patients (Fig. 2b) without an increase in spinal fractures is worrisome, especially since the SMR-protocol was implemented in order to decrease (secondary) neurological deterioration after spinal injuries. These findings suggest (secondary) detoriation has occurred after the initial trauma while the spine was immobilized, or possibly an improper or missing application of spinal immobilization was performed. In 2020, up to 10.0% of all admitted patients with spinal fractures suffered a TSCI, while this was 6% in 1986. However, the incidence for spinal fractures presented in the ED increased by almost 80.0%, but the admission rate for these patients decreased (Figs. 2c and 3). Nowadays, many trauma patients with neck/back pain will undergo a CT-scan. This might implicate that more minor fractures were found that did not require hospital admission or hospitalized care. Therefore the patient group that met the admission criteria for the database (LBZ/LMR) could have been changed and a relative increase in spinal fractures with TSCI could be expected. The clinical relevance of this significant increase in TSCI’s remains uncertain.
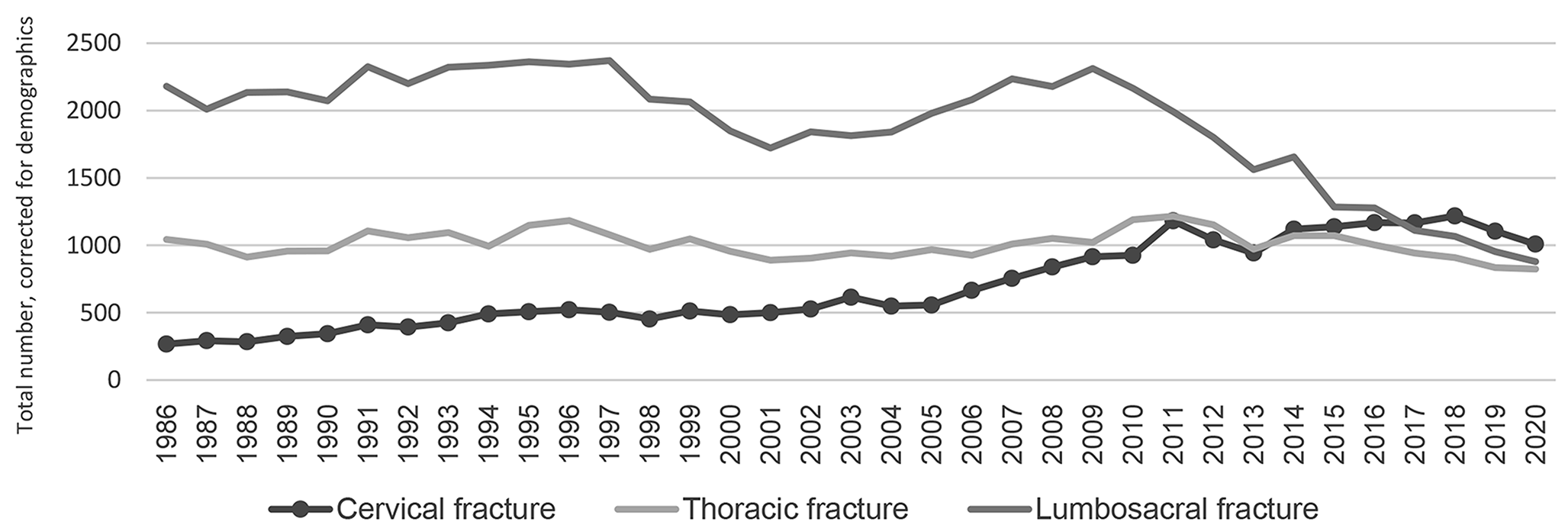
Furthermore, our study showed a notable difference between thoracic/lumbosacral fractures and cervical fractures within this study. TSCI in patients with lumbosacral or thoracic spinal fractures was observed in up to 5.0% of the patients, while the rate of cervical spinal fractures is much higher (up to 25.0%). In addition, during the study period the TSCI-incidence in thoracic/lumbosacral spinal fractures shows signs of decreasing at 5-year intervals, but in the group of patients with a cervical spinal fracture the TSCI-incidence no decrease is seen (Fig. 5). These findings might suggest the SMR-protocol helps preventing secondary (detoriation of) TSCI in thoracic and lumbosacral spinal fractures, but has less impact for the cervical spinal fractures. The admission-rate (Fig. 1) also shows that the admittance number rises for cervical fractures, whereas the admission-rate for thoracic spinal fractures remains even and lumbosacral spinal fractures declined over 50.0%. Given the higher mortality associated with TSCI located higher in the spinal cord, this highlights the importance of improving care for cervical fractures [29].
The results from this study should be interpreted with regard to its limitations. The inability to correct for confounders, such as changes in care and trauma systems that were not simultaneous implemented across all hospitals in the Netherlands, may impact the interpretation of the results. Although the use of a vacuum matress has been added to nationwide protocols in 2016, some EMS still use the obsolete long spinal board today [8, 9]. Second, The LIS-database started recording from 1997 which coincides with the introduction of the ATLS-protocol. The lack of detailed patient characteristics e.g. past medical history, comorbidities, medications) and outcomes (such as survival, treatment given, re-admissions) in both databases limits further in-depth analysis. In addition, spinal injuries with severe expected outcome are more likely to be reffered to the ED of level-1 trauma centers and injuries with a better prognosis are more likely to be referred to smaller, non-university level-2 hospitals. These existing referring logistics may affect the reliability of the LIS [24]. Furthermore, re-admitted patients might have been entered twice within the database, since re-admissions are not scored separately. However, to the best of our knowledge, this is the first review which evaluates the TSI/SMR-protocol by looking at the amount of reported neurological deficit after spinal fractures in The Netherlands. The system of data acquisiton and the LIS procedures have been unchanged during the study period, which allows for detection of trends.






留言 (0)