
記住我


Stroke is a major global health concern and is responsible for causing a substantial number of fatalities and disabilities (1). In recent years, China alone has reported millions of new stroke cases and related deaths (2). Critically ill stroke patients often experience reduced consciousness levels, severe dysphagia, and impaired gastrointestinal function, making them susceptible to malnutrition (3, 4). Malnourishment or nutritional vulnerability in stroke patients is associated with higher mortality rates, increased complications, and a poor functional prognosis (3–5). Guidelines suggest that critically ill stroke patients with reduced consciousness levels or prolonged severe dysphagia receive early enteral tube feeding within 72 h from the onset of symptoms (6, 7).
However, the optimal timing for initiating EN in severe stroke cases is still debated. Some studies have shown improved outcomes with early tube feeding within 7 days (8), while others suggest that initiating enteral nutrition within 3 days in comatose stroke patients does not improve nutritional status and may increase the likelihood of diarrhea (9). Consequently, this study aims to provide further insights into the relationship between the timing of enteral nutrition initiation and 28-day mortality in severe stroke patients, utilizing data from the MIMIC-IV database.
Methods Study populationThe present retrospective study utilized patient data from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) cohort, a single-center, longitudinal cohort spanning from 2008 to 2019. The MIMIC-IV database contains various patient information, including demographics, vital signs, laboratory results, diagnoses, medication details, and follow-up information. The data extraction code is available on GitHub (10) (http://github.com/MIT-LCP/mimic-iv). This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (11).
Inclusion and exclusion criteriaThis study included stroke patients, both ischemic and hemorrhagic, who received enteral nutrition (EN) during their initial ICU admission. Stroke diagnoses were based on ICD-9 or ICD-10 (International Classification of Disease, Ninth and Tenth Versions), with stroke consistently listed as the primary diagnosis. The inclusion criteria were as follows: (1) patients aged 18 years or older; (2) those with an ICU stay lasting 24 h or more; and (3) only patients in their initial ICU stay were considered. The exclusion criteria were as follows: (1) patients younger than 18 years, (2) patients with an ICU stay of fewer than 24 h, (3) patients with contradictions to enteral nutrition, such as gastrointestinal bleeding or intestinal obstruction, and (4) patients with a wait time for enteral nutrition beyond 15 days.
Data extractionStructured Query Language (SQL) was used for data extraction. The following variables, collected within 24 h of ICU admission, were extracted:
1. Patient's basic information: Sex, admission age, race, admission time, ICD code, EN start time, height, weight, body mass index (BMI), and 28-day mortality.
2. Vital signs: Temperature, mean blood pressure (MAP), heart rate, and SpO2.
3. Severity of illness scores: The Sequential Organ Failure Assessment (SOFA) score, the Simplified Acute Physiology Score II (SAPS II), the Glasgow Coma Scale (GCS), and the Charlson comorbidity index. If a patient was intubated and could not provide a verbal score for the GCS, it was estimated from the eye and motor scores, as reported in previous studies (12).
4. Laboratory test results: WBC count, creatinine levels, hematocrit (HCT), and albumin levels.
5. Treatment modalities: Mechanical thrombectomy and thrombolysis.
6. Commodities: Myocardial infarction, peripheral vascular disease, dementia, COPD, malignant cancer, renal disease, cancer, severe liver disease, gastrointestinal bleeding, or intestinal obstruction, identified by ICD codes.
Variable definition and outcomesEN initiation time was defined as the duration between the start of enteral nutrition (EN) and the time of ICU admission. We calculated the initiation time for various EN solutions, including Ensure, Impact, and Vivonex, among others. The main objective of this study was to investigate 28-day mortality as the primary outcome.
Statistical analysisBaseline patient characteristics were stratified based on different EN initiation time groups. Continuous data are expressed as either the mean ± standard deviation or median (inter-quartile), while categorical variables are expressed as numbers (percentages), as appropriate. Statistical comparisons between the two groups included the use of the chi-square test or Fisher's exact test for categorical variables, and continuous variables were examined using the analysis of variance test or rank-sum test.
We omitted the missing data for glucose levels, GCS, WBC, body weight, and creatinine due to the low percentage of missing data (missing rate below 5%). We also used multiple imputations to handle the missing data for BMI (missing rate: 34.9%) and serum albumin levels (missing rate: 47.8%).
We selected confounders based on clinical relevance and their association with the outcome (p < 0.2) or a change in effect estimate of more than 10%. Multivariable Cox regression models were introduced to evaluate the association between early EN initiation and 28-day mortality. Four models were employed in the regression analysis, each adjusted for different sets of variables:
Model 1: Adjusted for sex and admission age.
Model 2: Adjusted for stroke type, BMI, and GCS in addition to variables in Model 1.
Model 3: Adjusted for mechanical ventilation, the Charlson comorbidity index, serum albumin level, glucose, SAPS II, and MAP in addition to variables in Model 2.
Model 4: Adjusted for malignant cancer, diabetes, myocardial infarction, creatinine, WBC, platelets, HCT, thrombolysis therapy, and mechanical thrombectomy in addition to variables in Model 3.
To explore potential non-linear relationships between the timing of EN initiation and 28-day mortality, a restricted cubic spline (RCS) was utilized. Heterogeneity across subgroups was assessed using Cox regression analysis, and interactions were evaluated using a likelihood ratio test.
Statistical significance was determined using a two-tailed test with a threshold of P of < 0.05. All data analyses were conducted using the R software package (R version 4.0.3) and Free Statistics software version 1.7.
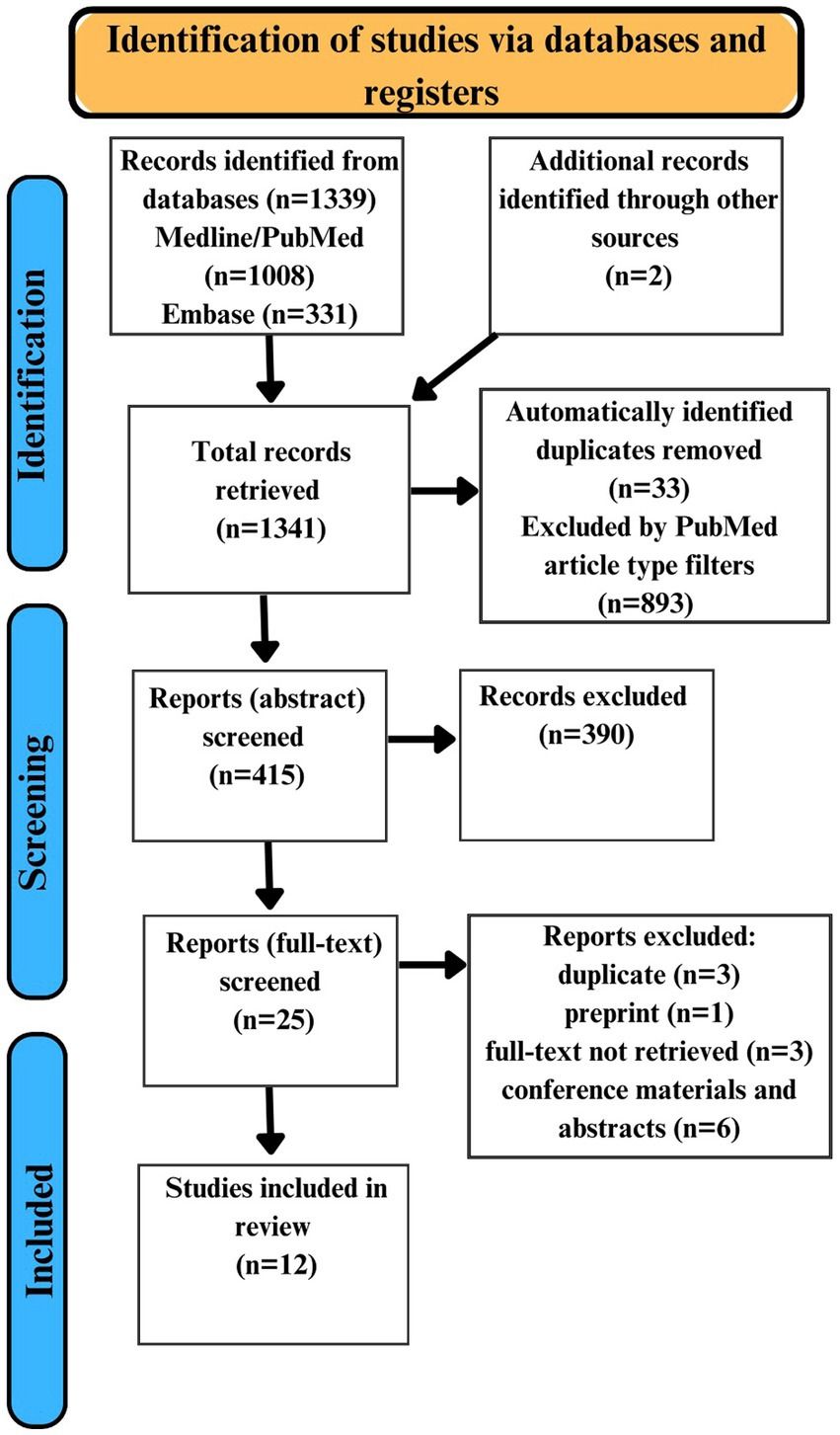
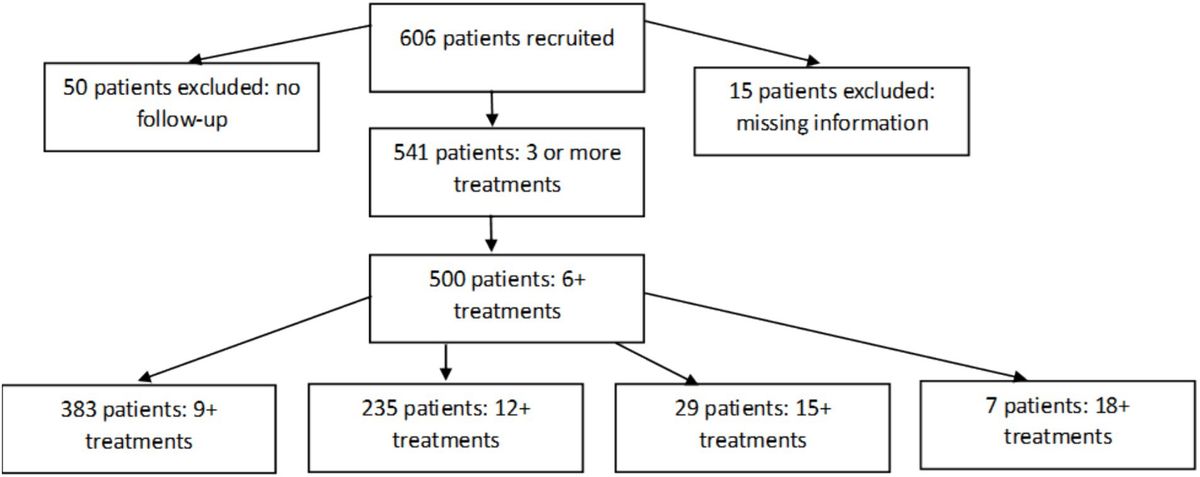
Results Baseline characteristicsA total of 10,051 individuals with a primary diagnosis of stroke, either ischemic or hemorrhagic, were identified and admitted to the ICU. Among them, 1,085 patients received enteral nutritional (EN) support. After excluding cases with outlier data (where the wait time for EN exceeded 15 days), contraindications, and missing data, our final cohort consisted of 997 stroke patients who received EN. Of these patients, 318 (31.9%) died within 28 days of their hospital admission. Figure 1 provides a detailed flowchart illustrating the participant recruitment process.
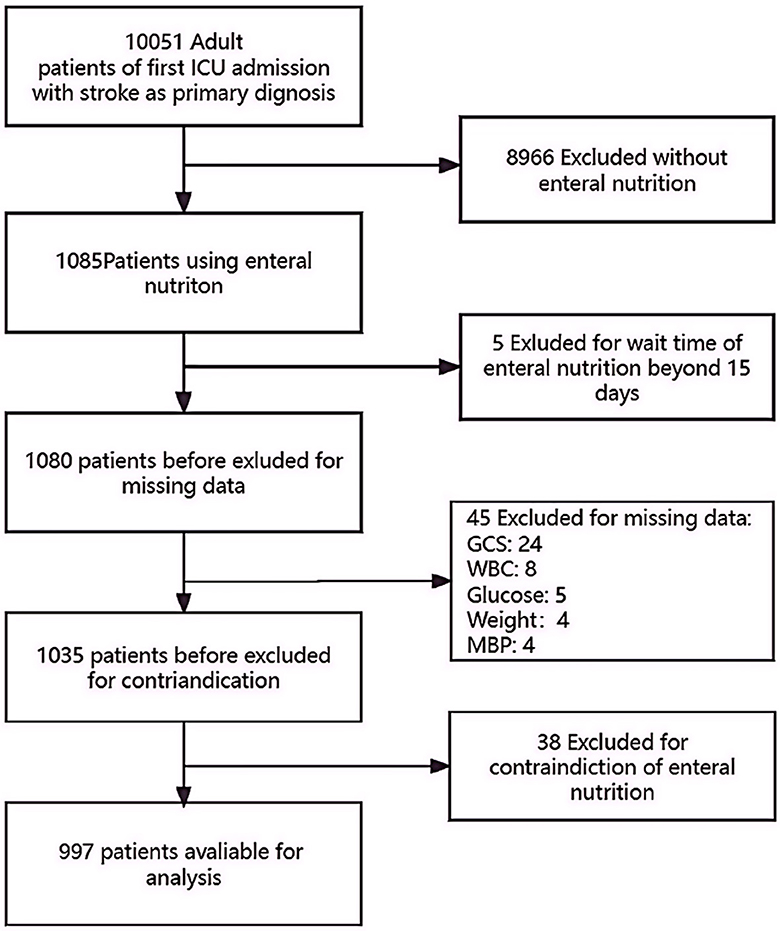
Figure 1. A detailed flowchart illustrating the participant recruitment process. GCS, Glasgow Coma Scale; WBC, white blood cell count; ICU, intensive care unit.
The average age of the 997 patients was 69.4 ± 14.6 years, and nearly half of them were women (49.9%). Table 1 presents the baseline characteristics of the included individuals. Compared to the late EN cohort, the early EN cohort had older patients, a higher prevalence of hemorrhagic stroke, a lower prevalence of mechanical ventilation, and lower admission albumin levels.
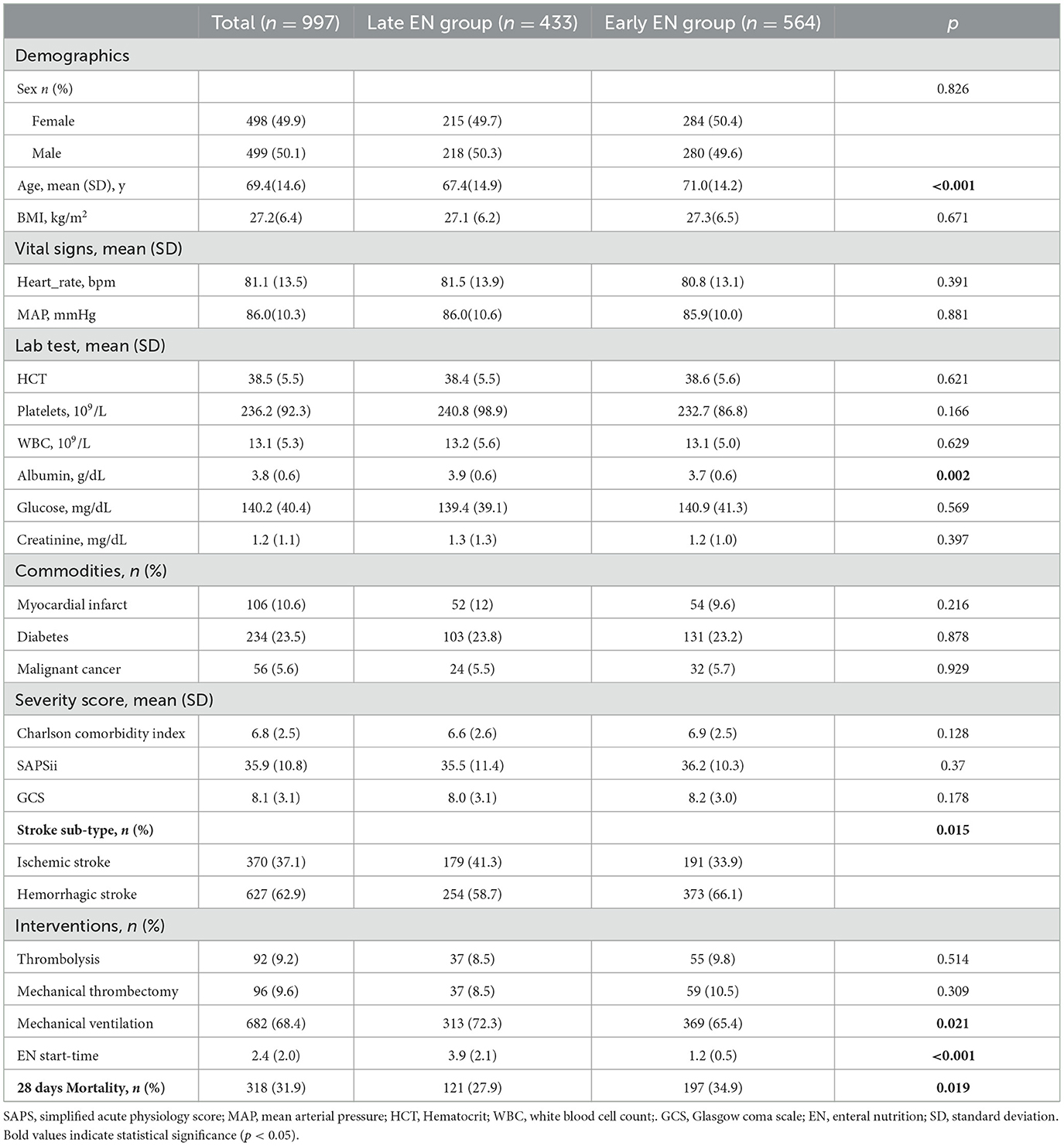
Table 1. Clinical information, and process parameters in patients categorized by EN start-time.
Effects of EN initiation time on 28-day mortalityIn our univariate Cox regression analysis (see Table 2), we observed a decline in 28-day mortality with increasing EN initiation time. Specifically, for each additional day of delay in EN initiation, there was a 6% decrease in the odds of death within 28 days [odds ratio (OR) = 0.94, 95% CI: 0.88–1, p = 0.044]. However, this correlation was not significant after adjusting for covariates.
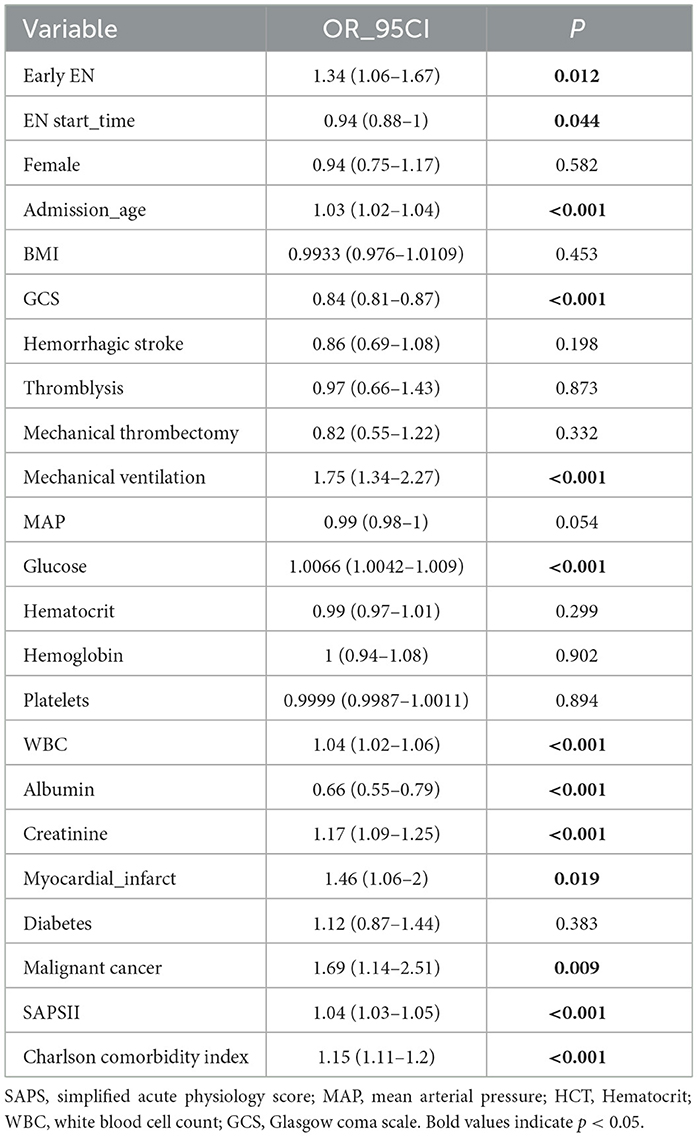
Table 2. Univariate logistic regression evaluating the association between baseline characteristic and 28 days-mortality.
On the other hand, the early EN group had a 34% higher mortality rate than the reference group (OR = 1.34, 95% CI: 1.06–1.67, p = 0.012). After adjusting for various confounding factors in the multivariable Cox models (see Table 3), we found that patients in the early EN group had a 27% higher risk of mortality than those in the reference group (OR = 1.27, 95% CI: 1.−1.61, p = 0.048).
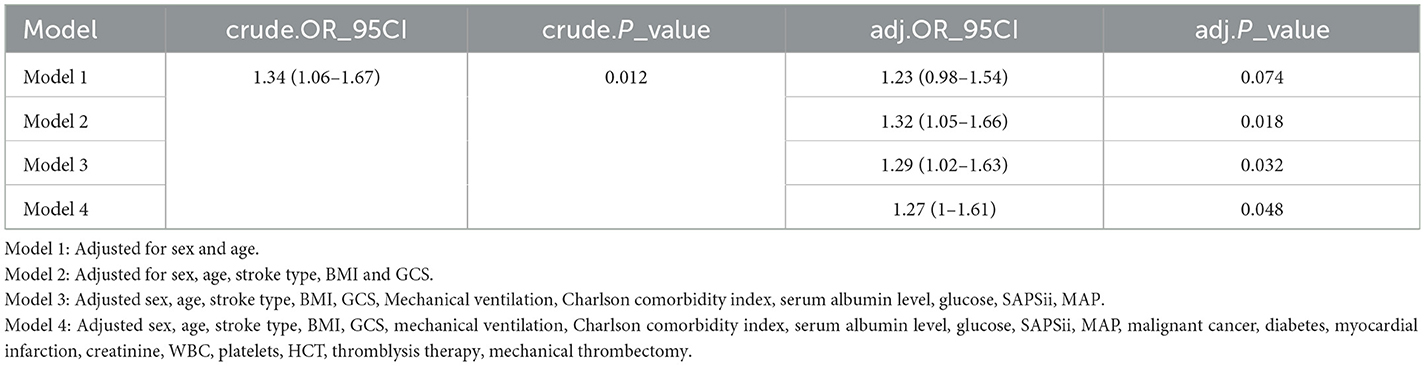
Table 3. Multivariable COX regression models evaluating the association between early EN and 28-days mortality.
We performed multivariable-adjusted restricted cubic spline analyses to further explore the association between EN initiation time and 28 days mortality. These analyses did not indicate a non-linear relationship between EN initiation time and mortality (as depicted in Figure 2).
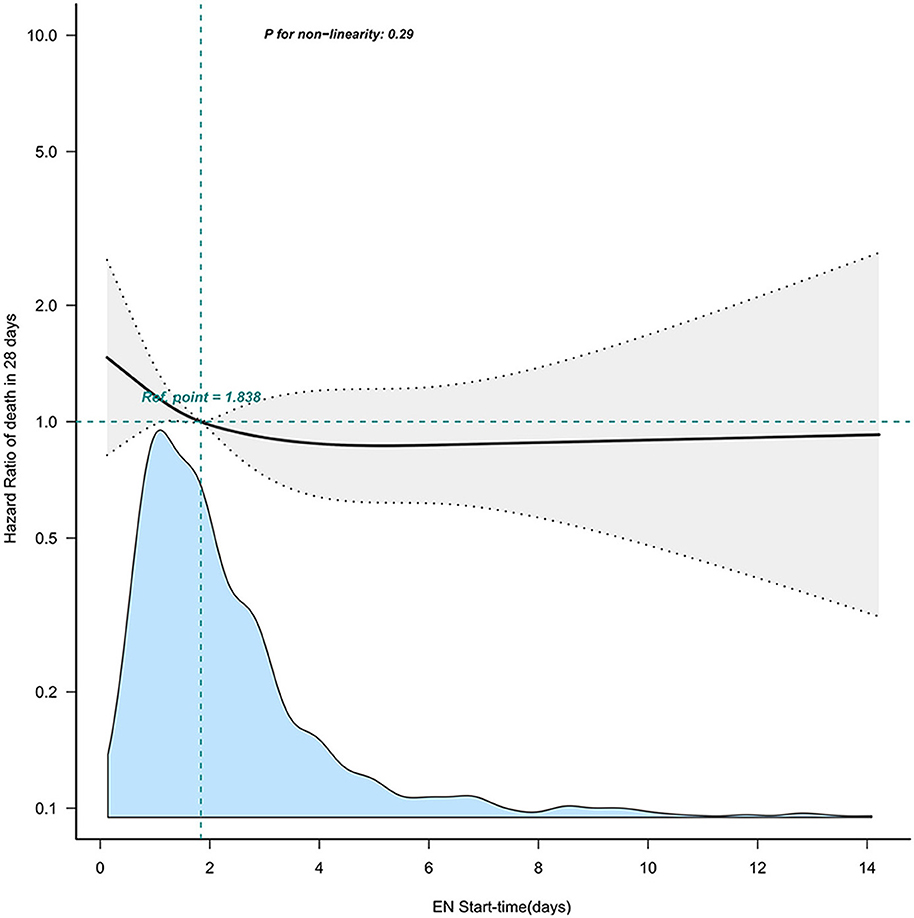
Figure 2. The non-linear relationship between EN start time and 28-day mortality. Adjusted confounders in model 4. This curve illustrates the mortality hazard of different EN start times within our cohort, using the median value of 1.8 days as a reference point. EN, enteral nutrition.
Survival analysis of these two groups showed that patients in the early EN group had poorer overall survival compared to those in the late EN group (p = 0.012) (Figure 3).
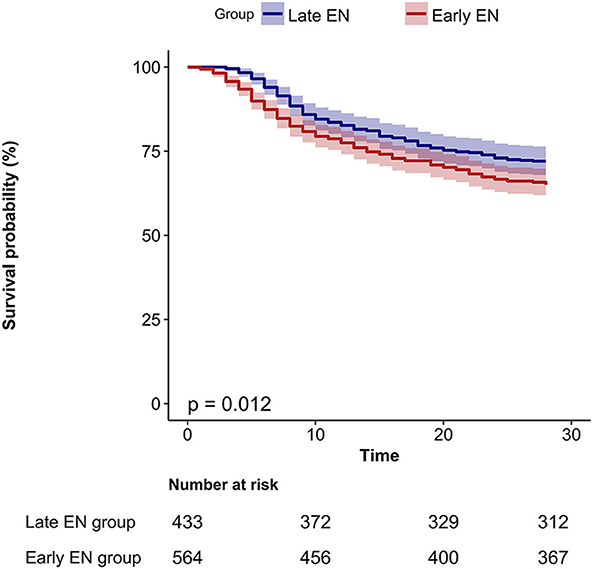
Figure 3. The K-M curve of survival in different EN (enteral nutrition) start time groups. EN, enteral nutrition.
Sensitivity analysisIn our multivariable Cox models, we meticulously adjusted for various confounding factors to assess the relationship between early EN initiation and 28-day mortality. Notably, the association remained consistent across all models (see Table 3). To further investigate the robustness of our findings, we conducted subgroup analyses based on various confounding factors such as age, sex, GCS, BMI, stroke type, thrombolysis, and thrombectomy (see Figure 4). We found a significant interaction in the subgroup of patients who underwent thrombolysis, which may be attributed to the small sample size in this group. No significant interactions were detected within any of the other subgroups (all p > 0.05) (Figure 4).
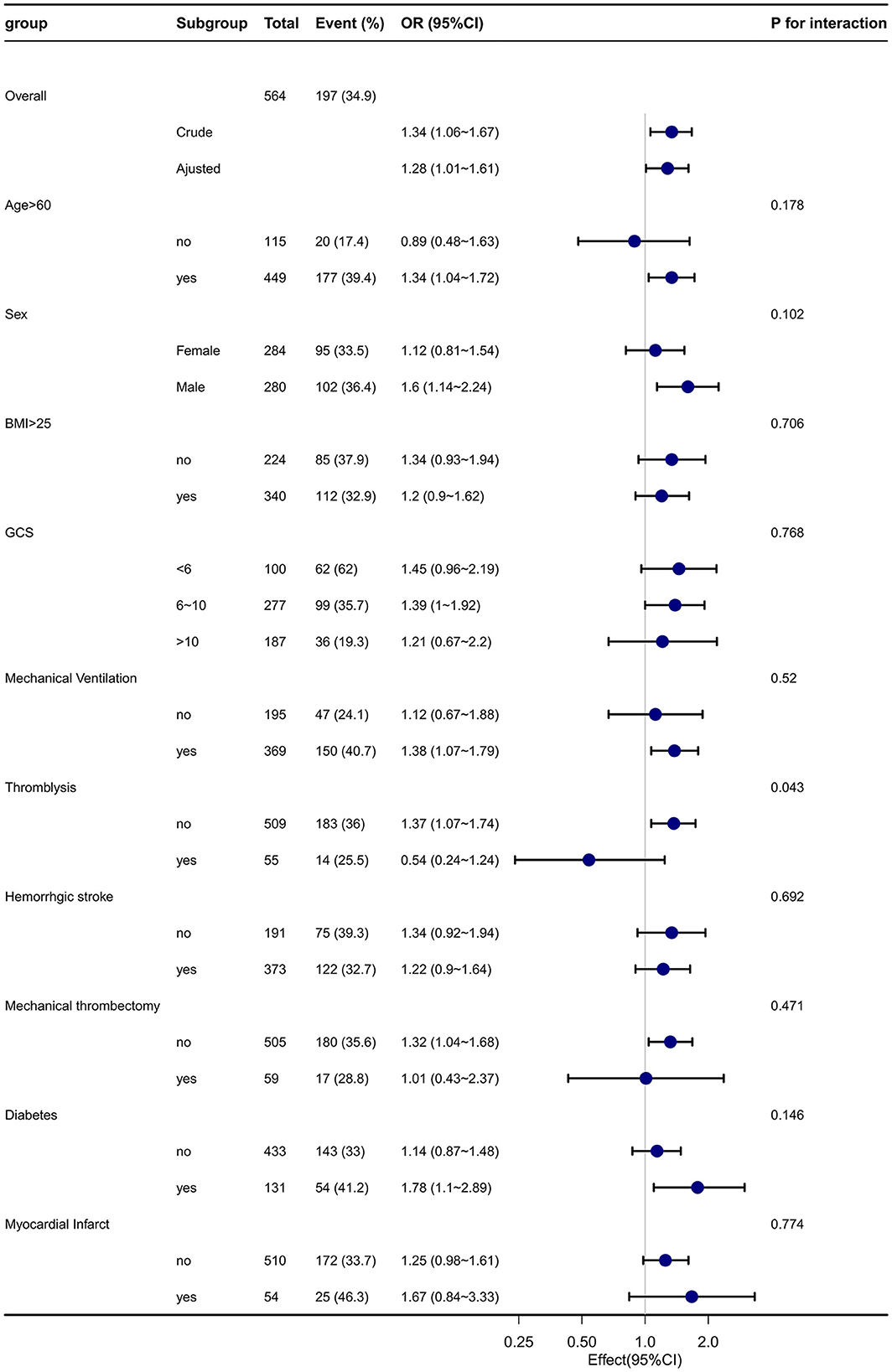
Figure 4. Effect size of early EN on 28-day mortality in each subgroup. A subgroup with varied demographics, including age, sex, Glasgow Coma Scale (GCS) scores, BMI, comorbidities such as diabetes and myocardial infarction, and different interventions, was analyzed within the early EN (enteral nutrition) group (n = 564), and the late EN (enteral nutrition) group (n = 433) was shown as a reference. The results from this subgroup analysis have demonstrated consistent and robust findings. GCS, Glasgow Coma Scale; WBC, white blood cell count; BMI, body mass index; SAPSii, Simplified Acute Physiology Score II; MAP: mean blood pressure Adjusted Charlson comorbidity index, SAPS II, MAP, creatinine, albumin, WBC, platelets, hematocrit, and glucose.
To mitigate potential bias, we redefined the early EN group as involving patients who started EN within the first day of admission (n = 211) and the late EN group as those who started EN after 1 day of admission (n = 768). After meticulous adjustments for various confounding factors in our multivariable Cox models, participants in the early EN group exhibited a higher risk of mortality (OR = 1.24, 95% CI: 0.96–1.61, p = 0.117) (Table 4).

Table 4. Multivariable COX regression model evaluating the association between early EN (in 1 day) and 28 days mortality.
We then divided the patients into four groups, EN within 1 day (n = 211), at 1–2 days (n = 353), 2–3 days (n = 209), and beyond 3 days (n = 224), to explore potential dose-response relationships. We found that that groups receiving EN in 2–3 days and beyond 3 days were associated with lower morality (all p < 0.05) compared to the early EN group (those receiving EN in 1 day), while the 1–2 days group did not show a significant difference in morality (p = 0.26) (Table 5).
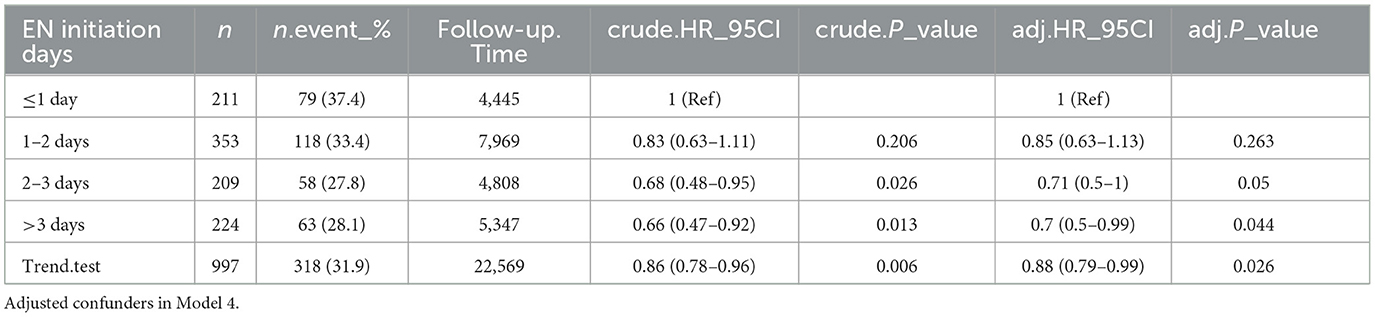
Table 5. Multivariable COX regression model evaluating the association between different EN initiation days and 28 days mortality.
DiscussionThis study primarily focused on investigating the correlation between the timing of enteral nutrition (EN) initiation and short-term outcomes in stroke patients admitted to the ICU. Our analysis revealed an independent correlation between EN initiation time and 28-day mortality, suggesting that starting EN within 2 days may be associated with higher mortality, which differs from mainstream views in this field of research.
These findings emphasize the crucial role of EN initiation timing in determining short-term outcomes for stroke patients receiving enteral nutrition in the ICU. It is essential to carefully consider the optimal time to initiate EN to minimize adverse outcomes. Early enteral nutrition (EN) offers advantages over total parenteral nutrition (TPN) in treating critically ill patients (13). It helps maintain gastrointestinal integrity, prevents intestinal bacterial translocation (14–19), and enhances recovery during the early hyper-metabolic stage (17, 19). It is evident from recent research that early EN is linked to positive outcomes, including lower mortality and fewer infectious complications, in patients with traumatic brain injury and intracranial hemorrhage (13, 18, 19).
However, it is crucial to emphasize that initiating intragastic feeding too early may result in elevated gastric load, hinder gastric emptying, and increase the chances of aspiration pneumonia in critically ill neurological patients (20). This finding has sparked significant debates regarding the ideal timing for commencing EN (21).
A recent meta-analysis comparing early parenteral nutrition (EPN) to early enteral nutrition (EEN) showed that EPN was more effective in lowering mortality and decreasing infectious complications in patients with acute gut-intolerant phase traumatic brain injuries (21). However, in the case of stroke patients, randomized controlled trials did not show any impact on mortality when comparing early and delayed EN (22).
Furthermore, a study conducted by Yamada et al. found that initiating enteral nutrition too early in comatose stroke patients may not provide nutritional advantages compared to early administration of total parenteral nutrition (TPN), and it might increase the risk of diarrhea (9).
Despite the limited number of studies addressing early EN and its impact on mortality, Cai et al. discovered that administering early EN within 48 h significantly reduced the occurrence of chronic hydrocephalus in severe intracranial hemorrhage patients (23). Similarly, Choi et al. reported that EEN within 72 h was associated with lower 28-day mortality and a reduced occurrence of infectious complications in critically ill neurological patients (24). It is worth noting that the definition of EEN varied among these studies, and our research specifically focused on stroke patients in ICUs.
The potential mechanisms underlying the increased 28-day mortality associated with EEN in critically ill stroke patients remain unclear. However, several possible explanations can be speculated upon. First, initiating early intro-gastric feeding has been associated with an increased likelihood of experiencing gastric complications and developing aspiration pneumonia in critically ill patients with brain injuries (20). These complications can negatively affect patient outcomes and contribute to the observed increase in mortality.
Second, the sympathetic hyperactivation resulting from increased intracranial pressure caused by a stroke can negatively affect gastrointestinal function (25–27). This disruption in the autonomic nervous system may interfere with proper gastrointestinal functioning, leading to complications and potentially higher mortality rates in stroke patients receiving EEN.
Additionally, when comparing EPN and EEN in patients with traumatic brain injuries, research has indicated that EPN is more effective in reducing mortality and infectious complications during the acute gut-intolerant phase (21). This finding suggests that the choice of feeding method can significantly impact patient outcomes, and in certain critical conditions, EEN may not be as effective.
Strengths and limitationsOur study boasts several strengths. First, it investigated the association between early enteral nutrition (EN) start time and 28-day mortality in stroke patients admitted to the ICU, providing novel insights into the field. We used RCS to test for non-linear correlations between EN start time and outcomes, which contributed valuable information for the development of EN therapy management strategies for this patient population.
Second, we conducted multiple sensitivity analyses to ensure robustness. Subgroup analyses were conducted based on stroke subtypes, age, sex, GCS score, and thrombolytic/thrombectomy therapy. The consistent results across these subgroups indicate that the relationship between EN initiation time and 28-day mortality remains independent of these factors. An interaction was found in the subgroup of thrombolysis, which may be due to the small sample size, this interaction requires further investigation. Additionally, our Cox regression analyses, adjusted across multiple models, accounted for confounding factors and validated the robustness of the outcomes.
However, our study has limitations. First, the unavailability of the National Institutes of Health Stroke Scale (NIHSS) score in the MIMIC-IV database prevented its inclusion as an important predictor of stroke severity (9). Nonetheless, the GCS score served as an alternative measure of neurological function.
Second, during the wait time for EN, only five patients receive TPN in our cohort, and we did not account for TPN in our analysis. Additionally, the calories received before EN could not be acquired from the MIMIC-IV database.
Third, detailed information such as whether EN feeding was successful was difficult to obtain from the MIMIC-IV database, even though the success rate of feeding is an important factor in 28-day mortality. This limitation could introduce bias into our findings.
Fourth, our study was limited to the United States and a single ICU institution, potentially impacting the generalizability of the findings. Different healthcare settings and practices might influence the applicability of the findings. Future prospective multicenter studies could help validate these results in a more diverse patient population.
Finally, considering that a particular stroke population (9.9%) was analyzed, there may be a selection bias that could affect the results. Conducting future randomized controlled trials would provide more robust evidence to validate these findings.
ConclusionIn conclusion, this study revealed an increased risk of 28-day mortality when EN was initiated within the first 2 days for stroke patients admitted to the ICU. Further research is imperative to understand the significance of this association. Subsequent research confirming these findings could establish a theoretical basis for delineating a specific time window to implement targeted nutritional therapy strategies for stroke patients.
Data availability statementThe data utilized in this study were obtained from the Medical Information Mart for Intensive Care IV (MIMIC-IV) Clinical Database (28). Requests for access to these datasets could be directed to PhysioNet (29, 30) and the raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementEthical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributionsXW: Writing – original draft, Software, Investigation, Formal Analysis, Data curation, Conceptualization. XXi: Writing – original draft, Visualization, Supervision, Resources, Investigation, Formal Analysis, Data curation. XXu: Writing – review & editing, Visualization, Validation, Supervision. LT: Writing – review & editing, Validation, Supervision, Methodology, Conceptualization.
FundingThe author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
AcknowledgmentsWe thank the Free Statistics team for their unselfish assistance and encouragement.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AbbreviationsMIMIC-IV, Medical Information Mart for Intensive Care-IV; EN, Enteral nutrition; ICU, Intensive care unit; NIHSS, National Institutes of Health Stroke Scale; GCS, Glasgow Coma Scale; TPN, Total parenteral nutrition; EPN, Early parenteral nutrition; EEN, Early enteral nutrition; WBC, White blood cell; SASPII, Simplified Acute Physiology Score II; BMI, Body mass index; SQL, Structured Query Language; MAP, Mean blood pressure; SOFA, Sequential Organ Failure Assessment score; BUN, Blood urea nitrogen; SD, Standard deviation.
References1. Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, et al. Heart disease and stroke statistics-2023 Update: a report From the American Heart Association. Circulation. (2023) 147:e93–e621. doi: 10.1161/CIR.0000000000001123
PubMed Abstract | Crossref Full Text | Google Scholar
2. Wang YJ Li ZX, Gu HQ, Zhai Y, Zhou Q, Jiang Y, et al. China Stroke Statistics: an update on the 2019 report from the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations. Stroke Vasc Neurol. (2022) 7:415–50. doi: 10.1136/svn-2021-001374
PubMed Abstract | Crossref Full Text | Google Scholar
3. Burgos R, Bretón I, Cereda E, Desport JC, Dziewas R, Genton L, et al. ESPEN guideline clinical nutrition in neurology. Clin Nutr. (2018) 37:354–96. doi: 10.1016/j.clnu.2017.09.003
PubMed Abstract | Crossref Full Text | Google Scholar
4. Sung SF, Chen YW, Tseng MC, Ong CT, Lin HJ. Atrial fibrillation predicts good functional outcome following intravenous tissue plasminogen activator in patients with severe stroke. Clin Neurol Neurosurg. (2013) 115:892–5. doi: 10.1016/j.clineuro.2012.08.034
PubMed Abstract | Crossref Full Text | Google Scholar
5. Lee ZY, Noor Airini I, Barakatun-Nisak MY. Relationship of energy and protein adequacy with 60-day mortality in mechanically ventilated critically ill patients: a prospective observational study. Clin Nutr. (2018) 37:1264–70. doi: 10.1016/j.clnu.2017.05.013
PubMed Abstract | Crossref Full Text | Google Scholar
6. Wirth R, Smoliner C, Jager M, Warnecke T, Leischker AH, Dziewas R, et al. Guideline clinical nutrition in patients with stroke. Exp Transl Stroke Med. (2013) 5:14. doi: 10.1186/2040-7378-5-14
PubMed Abstract | Crossref Full Text | Google Scholar
8. Collaboration FT. Poor nutritional status on admission predicts poor outcomes after stroke: observational data from the FOOD trial. Stroke. (2003) 34:1450–6. doi: 10.1161/01.STR.0000074037.49197.8C
PubMed Abstract | Crossref Full Text | Google Scholar
9. Yamada SM. Too early initiation of enteral nutrition is not nutritionally advantageous for comatose acute stroke patients. J Nippon Med Sch. (2015) 82:186–92. doi: 10.1272/jnms.82.186
PubMed Abstract | Crossref Full Text | Google Scholar
10. Johnson AE, Stone DJ, Celi LA, Pollard TJ. The MIMIC Code Repository: enabling reproducibility in critical care research. J Am Med Inform Assoc. (2018) 25:32–9. doi: 10.1093/jamia/ocx084
PubMed Abstract | Crossref Full Text | Google Scholar
11. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med. (2007) 4:e297. doi: 10.1371/journal.pmed.0040297
PubMed Abstract | Crossref Full Text | Google Scholar
12. Meredith W, Rutledge R, Fakhry SM, Emery S, Kromhout-Schiro S. The conundrum of the Glasgow Coma Scale in intubated patients: a linear regression prediction of the Glasgow verbal score from the Glasgow eye and motor scores. J Trauma. (1998) 44:839–44; discussion 44–5. doi: 10.1097/00005373-199805000-00016
PubMed Abstract | Crossref Full Text | Google Scholar
13. Kattelmann KK, Hise M, Russell M, Charney P, Stokes M, Compher C. Preliminary evidence for a medical nutrition therapy protocol: enteral feedings for critically ill patients. J Am Diet Assoc. (2006) 106:1226–41. doi: 10.1016/j.jada.2006.05.320
PubMed Abstract | Crossref Full Text | Google Scholar
14. Chiang YH, Chao DP, Chu SF, Lin HW, Huang SY, Yeh YS, et al. Early enteral nutrition and clinical outcomes of severe traumatic brain injury patients in acute stage: a multi-center cohort study. J Neurotrauma. (2012) 29:75–80. doi: 10.1089/neu.2011.1801
PubMed Abstract | Crossref Full Text | Google Scholar
15. Chourdakis M, Kraus MM, Tzellos T, Sardeli C, Peftoulidou M, Vassilakos D, et al. Effect of early compared with delayed enteral nutrition on endocrine function in patients with traumatic brain injury: an open-labeled randomized trial. J Parent Enteral Nutr. (2012) 36:108–16. doi: 10.1177/0148607110397878
PubMed Abstract | Crossref Full Text | Google Scholar
17. Reintam Blaser A, Starkopf J, Alhazzani W, Berger MM, Casaer MP, Deane AM, et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intens Care Med. (2017) 43:380–98. doi: 10.1007/s00134-016-4665-0
PubMed Abstract | Crossref Full Text | Google Scholar
18. Ohbe H, Jo T, Matsui H, Fushimi K, Yasunaga H. Early enteral nutrition in patients with severe traumatic brain injury: a propensity score-matched analysis using a nationwide inpatient database in Japan. Am J Clin Nutr. (2020) 111:378–84. doi: 10.1093/ajcn/nqz290
PubMed Abstract | Crossref Full Text | Google Scholar
19. Cheng X, Ru W, Du K, Jiang X, Hu Y, Zhang W, et al. Association between enteral nutrition support and neurological outcome in patients with acute intracranial haemorrhage: a retrospective cohort study. Sci Rep. (2019) 9:16507. doi: 10.1038/s41598-019-53100-w
PubMed Abstract | Crossref Full Text | Google Scholar
20. Acosta-Escribano J, Fernández-Vivas M, Grau Carmona T, Caturla-Such J, Garcia-Martinez M, Menendez-Mainer A, et al. Gastric versus transpyloric feeding in severe traumatic brain injury: a prospective, randomized trial. Intens Care Med. (2010) 36:1532–9. doi: 10.1007/s00134-010-1908-3
PubMed Abstract | Crossref Full Text | Google Scholar
21. Wang X, Dong Y, Han X, Qi XQ, Huang CG, Hou LJ. Nutritional support for patients sustaining traumatic brain injury: a systematic review and meta-analysis of prospective studies. PLoS ONE. (2013) 8:e58838. doi: 10.1371/journal.pone.0058838
PubMed Abstract | Crossref Full Text | Google Scholar
22. Dennis MS, Lewis SC, Warlow C. Effect of timing and method of enteral tube feeding for dysphagic stroke patients (FOOD): a multicentre randomised controlled trial. Lancet. (2005) 365:764–72. doi: 10.1016/S0140-6736(05)17983-5
PubMed Abstract | Crossref Full Text | Google Scholar
23. Cai Z, Zhao K, Li Y, Wan X, Li C, Niu H, et al. Early enteral nutrition can reduce incidence of postoperative hydrocephalus in patients with severe hypertensive intracerebral hemorrhage. Med Sci Monit. (2022) 28:e935850. doi: 10.12659/MSM.935850
PubMed Abstract | Crossref Full Text | Google Scholar
24. Choi YK, Kim HJ, Ahn J, Ryu JA. Impact of early nutrition and feeding route on clinical outcomes of neurocritically ill patients. PLoS ONE. (2023) 18:e0283593. doi: 10.1371/journal.pone.0283593
PubMed Abstract | Crossref Full Text | Google Scholar
25. Patejdl R, Kästner M, Kolbaske S, Wittstock M. Clinical nutrition and gastrointestinal dysfunction in critically ill stroke patients. Neurol Res. (2017) 39:959–64. doi: 10.1080/01616412.2017.1367545
PubMed Abstract | Crossref Full Text | Google Scholar
26. Liff JM, Labovitz D, Robbins MS. Profound gastroparesis after bilateral posterior inferior cerebellar artery territory infarcts. Clin Neurol Neurosurg. (2012) 114:789–91. doi: 10.1016/j.clineuro.2011.12.042
PubMed Abstract | Crossref Full Text | Google Scholar
27. Walter U, Kolbaske S, Patejdl R, Steinhagen V, Abu-Mugheisib M, Grossmann A, et al. Insular stroke is associated with acute sympathetic hyperactivation and immunodepression. Eur J Neurol. (2013) 20:153–9. doi: 10.1111/j.1468-1331.2012.03818.x
PubMed Abstract | Crossref Full Text | Google Scholar
28. Johnson AEW, Bulgarelli L, Shen L, Gayles A, Shammout A, Horng S, et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci Data. (2023) 10:1. doi: 10.1038/s41597-023-02136-9
PubMed Abstract | Crossref Full Text | Google Scholar
29. Johnson A, Bulgarelli L, Pollard T, Horng S, Celi LA, Roger M. MIMIC-IV. PhysioNet (2023).
留言 (0)