
記住我



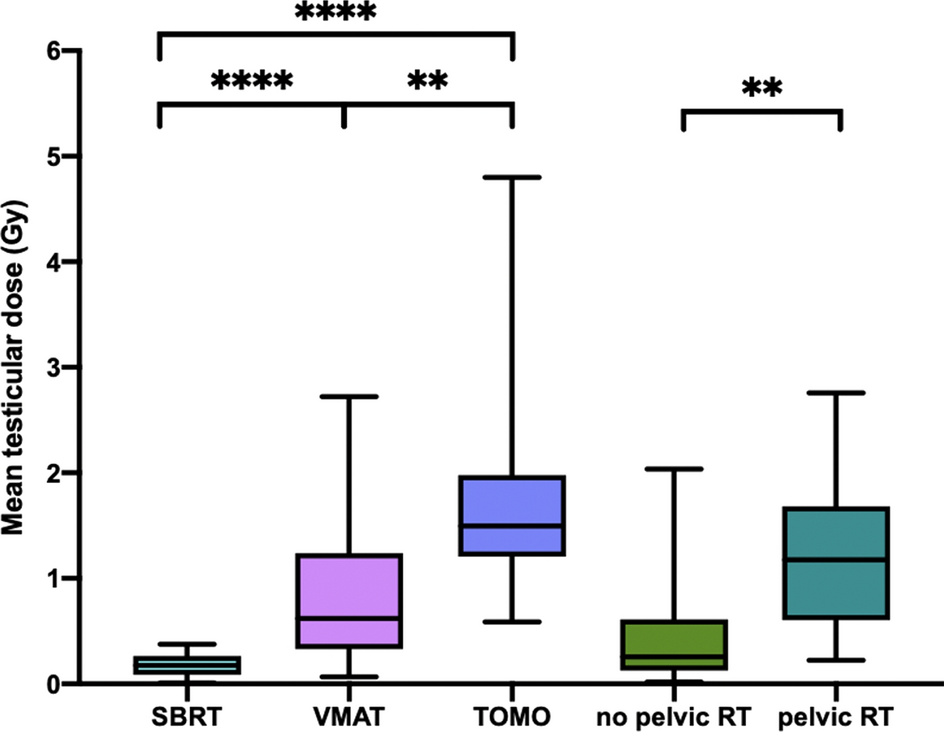
Our study showed that testicular dose delivered by modern radiotherapy techniques during a standard prostate irradiation is not negligible, with a median dose of 0.58 Gy. Tomotherapy, pelvic nodal irradiation and lower BMI were significantly associated with increased median testicular dose.
Testis is one of the most radiosensitive tissues in humans and especially spermatogonia stem cells. Numerous studies have reported the impact on sperm count of incidental irradiation for testicular seminoma, Hodgkin disease, thyroid cancer (131I ablation) or rectal cancer. Doses as low as 0.15 Gy have been described to produce reduction in sperm count and temporary azoospermia occurs for doses over 0.3 Gy [8, 9]. The doses of irradiation required to kill spermocytes and spermatids are higher than spermatogonia (2–3 Gy and 4–6 Gy respectively). After low dose testis irradiation, spermatogonia, spermatocytes, and, ultimately, spermatids disappear from the testis. Since the combined life span of spermatocytes and spermatids is about 46 days and transport through the epididymis and vas deferens takes 4–12 days, sperm production is maintained during the first 50–60 days and then drops dramatically with resultant temporary oligo- or azoospermia [18, 19]. The nadir of sperm count occurs 4–6 months after the end of treatment, and complete recovery requires 10–18 months after less than 1 Gy, 30 months for 2–3 Gy, and 5–10 or more years after 4–6 Gy since germinal epithelium seems to been damaged at this dose range [9, 18, 20,21,22]. Doses above 1.2 Gy have been associated with a reduced risk of recovery of spermatogenesis [23]. Cumulative doses of fractionated radiotherapy more than 2–2.5 Gy generally result in prolonged and likely permanent azoospermia [9, 24,25,26].
Our cohort indicated that many patients could face fertility impairment post-EBRT, despite using modern techniques. Notably, 84% of patients reached the oligospermia theoretical dose threshold, and 65% reached the azoospermia dose threshold. 29% received an average testicular dose above 1.2 Gy (dose associated with reduced chance of spermatogenesis recovery in literature) and 10% exceeded 2 Gy (associated with a risk ofpermanent azoospermia) (Fig. 4).
Fig. 4
proportion of patients in the cohort meeting the testicular dose threshold for oligospermia, temporary azoospermia, and definitive azoospermia with a modern prostate cancer radiotherapy plan
Beyond the impact on spermatozoid production, some studies reported a long-term impact of prostate cancer EBRT on hormone levels [27,28,29]. Leydig cells are reputed less radiosensitive then spermatogonial stem cells but negative effects have been reported after 2 Gy [9, 23, 30]. In a study on 33 men, serologic evaluation for hypogonadism was undertaken three to eight years after primary EBRT treatment for localized prostate carcinoma and was compared with 55 similar men who had received radical prostatectomy (none had undergone hormonal treatment since primary therapy). In the EBRT group, total testosterone levels averaged 27.3% less, luteinizing hormone (LH) levels 52.7% greater, and follicle-stimulating hormone (FSH) levels 100% greater [28]. However, in Tomić, Grigsby and Daniell studies [27,28,29], radiation technique were ancient and estimated dose to testicle was high (from 1 to 10 Gy for instance in Tomić’s study) so one can suppose that the hormonal impact of modern radiotherapy may be lower. So far, there is no evidence about the precise dose range in which hormonal impairment remains as a permanent side effect of irradiation [30].
Our study is, to the best of our knowledge, the only one reporting testicular dose with modern radiotherapy techniques. One can see that the dose reported in our study seems lower than what used to be delivered with 2D or 3D techniques. For instance, a prediction of a four-field treatment 3D radiotherapy on an anthropomorphic phantom in 17 patients indicates that testicular doses may be estimated with 1–2% of the tumor dose (range 0.4–2.2%), being about 1 Gy for a 80 Gy prescription [31]. In Boehmer et al.’s study, the calculated projected doses received by the unshielded testicles during a course of 20-MV conventional external-beam radiotherapy on a standard series of 40 fractions of external-beam radiotherapy for patients with localized prostate cancer were 1.96 Gy (± 1.45 Gy) [30]. Indeed, during the 2D/3D era, the clinical volumes were larger than what we can define nowadays with prostate magnetic resonance imaging (MRI) and the setup margins were also larger because of greater repositioning uncertainties with 2D imaging compared with Cone Beam Computed Tomography (CBCT).
Although it has not been proven in humans, some studies showed in animals that fractionated irradiation of the testes is more harmful than single treatments, at least up to total doses of about 6 Gy [20, 24]. Extremely hypofractioned treatments such as the ones allowed by stereotactic radiotherapy may reduce the fertility impact, all the more since their steep dose gradient deliver significantly lower dose to testicles compared with VMAT and Tomotherapy (median 0.18 Gy in our study). However, one should be careful when using stereotactic radiotherapy with non-coplanar beams such as Cyberknife for instance, since the entrance of the beams can be directly through the testicles and the radiation oncologist should take this in consideration when checking dosimetry. Moreover, our study showed that tomotherapy should be avoided in younger prostate cancer patients with a parenthood desire, since one fourth of the patients in our cohort received more than 2 Gy in average to testicles with this technique, despite the use of TomoEdge. The TomoEdge technology enables the superior and inferior jaw to open and close independently at the start and end of a target in order to reduce the longitudinal penumbra [32]. Without this feature, the dose to testicles might be far greater. Certainly, the radiation dose may be even more reduced by using even more advanced radiotherapy techniques such as proton therapy. Indeed, in one study on 16 men with low- or intermediate-risk prostate cancer treated with proton therapy, only one was found to have oligospermia indicating minimal scatter radiation to the testis during treatment. There was however a statistically significant reduction in semen volume and increase in pH [33].
Moreover, lead shields are not routinely used in prostate radiotherapy and yet they have been proven to reduce testicular dose in 3D techniques [27]. The gonadal shield allows a two to tenfold reduction in dose to the testes depending primarily on the distance from the field edge to the gonads [34]. In a study reporting the testicular dose using in vivo measurements in 16 men with testicular seminoma receiving abdominopelvic radiation therapy (modified dog-leg field) with anteroposterior/posteroanterior parallel-opposed photon beams with and without gonadal shielding, the mean measured dose to the testis in the patients with gonadal shielding was 0.03 Gy compared with 0.3 Gy in the unshielded group for a 25 Gy treatment [35]. However, testicular dose results from both leakage from the primary source as well as internal scatter and testicular shielding reduces only the dose from the primary source but not the internal scatter part.
The best technique to reduce testicular dose in a radical primary treatment for localized prostate cancer remains surely brachytherapy given its incomparable dose gradient. In a study following four young prostate cancer patients after brachytherapy with a total estimated dose to testis of 0.2 Gy, no significant change in semen parameters were found post-therapy and three of them were able to father a child subsequently without any deleterious side‐effects [36]. Huyghe’s team has one of the most important experiences in fertility after prostate brachytherapy. Among the 122 men under 65 years old treated by brachytherapy, four men manifested a fatherhood desire. One year after brachytherapy, their spermogram showed a low ejaculatory volume and a moderate asthenospermia but had a rich sperm count, compatible with a spontaneous pregnancy [37]. However, due to the prolonged half-life of the isotopes used, attempts at conception have to be delayed for up to 3 to 12 months after treatment [36, 38].
The issue of fertility preservation in prostate cancer patients is sometimes overlooked because of misconceptions from medical staff of a “limit” age to be a father. However, in a survey in 115 men treated for prostate cancer, all patients stated that they were informed of the incontinence and impotence side effects of the treatments, but only 8.7% stated that they were informed of the effect on their future fertility while 3.7% listed fertility as their major concern [39].
As reminded in the recent European Society for Medical Oncology (ESMO) recommendations on fertility preservation, sperm cryopreservation before initiation of anticancer treatments (chemotherapy, radiotherapy or surgery) is standard of care and should be discussed with any male cancer patient at risk of infertility [40]. If azoospermia is discovered after radiation therapy in a patient that has a paternity desire, the only possibility to harvest spermatozoa is through in invasive procedure (deferential, epididymal or testicular sperm extraction) and IntraCytoplasmic Sperm Injection (ICSI) [9, 41]. Pretreatment semen cryopreservation is safer, cheaper and generally results in more sperm for future use than postoperative surgical retrieval. Moreover, our results showed that patients requiting pelvic irradiation were the ones receiving the highest dose to testicles and those patients usually requires hormone deprivation therapy, from 6 months up to 3 years, with a testosterone recuperation that may take months or even years [42]. This will likely push these patients into an age range where testis recovery is rather moot and spermatogenesis naturally declines after 40 years old [43]. Ideally, the situation should be anticipated and discussed before any specific treatment, to favor pretreatment semen cryopreservation. An appropriate pre-treatment counseling in a center specialized in fertility issues is advisable.
The limitations of our study are of course its retrospective nature, its relatively low numbers and the lack of correlation with post-treatment fertility data such as hormonal and semen analyses or ulterior successful pregnancies. However, given the relatively low incidence of cancer prostate in young patients in each radiotherapy center, the feasibility of such a prospective study with sperm counts is unrealistic. The mean age of the patients included in this dosimetric study was also much higher than patients usually concerned with fertility issues but there is no reason why the dose to testicles would be different. Indeed, the dose to the testicles in our study was not significantly associated with age. The radiation doses threshold data and their semenanalysis outcomes used in this study were primarily in younger patients. It is not known if radiation therapy is more or less of a risk to the younger, developing testis or the older testis. Furthermore, emerging data suggests that spermatogenesis declines slowly after age 40 [43], so it is unclear if at these advanced paternal ages radiotherapy really will impact the testis that may have already declined.
Neither of the plans was optimized to deliver the lowest dose possible to testicle since it is not performed in routine care. Yet, modern radiotherapy techniques allow for inverse planning and optimization, providing the organ at risk is contoured and a constraint is set on it. However, clinically meaningful doses to testicles being very low, it is probable that a mere optimization won’t decrease testicular dose in a significant way. Also, modern commercial TPS allow for a testicular dose estimation although they tend to underestimate the out-of-field dose, up to 60% in mean dose to organs located beyond the 2% isodose [44,45,46,47]. A Monte Carlo simulation or direct measurements are precise but are so time-consuming that they are impractical for routine clinical use [44]. Modern radiotherapy also includes Image Guided RadioTherapy (IGRT). The dose delivered with imaging has historically been discarded because of its negligible contribution compared with therapeutic dose, in the era of 2D imaging. However, modern prostate radiotherapy requires a simulation CT scan for dosimetry and usually a CBCT at each fraction for an accurate repositioning since it was proven to improve outcomes in prostate cancer [48]. The limit of our study is that the dose delivered by daily positioning images was not recorded, and yet it is not negligible with daily CBCTs, especially when considering organs with very low dose tolerance [49]: about 0.8 Gy to testicles for 40 fractions for a pelvic treatment [50] and the typical imaging dose is approximately 1.5 cGy per image in Tomotherapy (0.6 Gy for a whole 40-fractions treatment considering one CBCT per fraction) [51]. A solution could be to reduce CBCT frequency, notably with moderate or ultra-hypofractionation. MR-guided radiotherapy is also a way to avoid the low doses delivered with repositioning imaging. The variability of techniques, equipment and field sizes used in our study also introduce a degree of heterogeneity in the cohort that cannot be accounted for. The latter limitations show that the testicular dose we estimated in our cohort and more generally in clinical practice is underestimated and the rate of clinically meaningful impact on fertility is probably higher than we could expect.
Our study shows that even with modern techniques, the dose delivered to testicles during a prostate radiotherapy is far from negligible, especially when pelvic nodes are treated or when a Tomotherapy technique is used. This dose could probably be reduced with optimized patient positioning to increase the distance between testicles and radiotherapy fields. Above all, SBRT and brachytherapy should be favored in younger patients in this consideration when suitable. Patients are often ill-informed and yet concerned with the potential impacts that the cancer treatments may have on their fertility. Given the difficulties that one can foresee to retrieve spermatozoa after a prostate radiotherapy, the ideal situation is to offer fertility counseling and sperm cryopreservation before any treatment to the fraction of patients who may still have a paternity desire.
留言 (0)