In this section epidemiological trends, severe outcomes and risk factors of common organisms causing bacteraemia in tropical settings will be discussed.
Staphylococcus aureus Bacteraemia
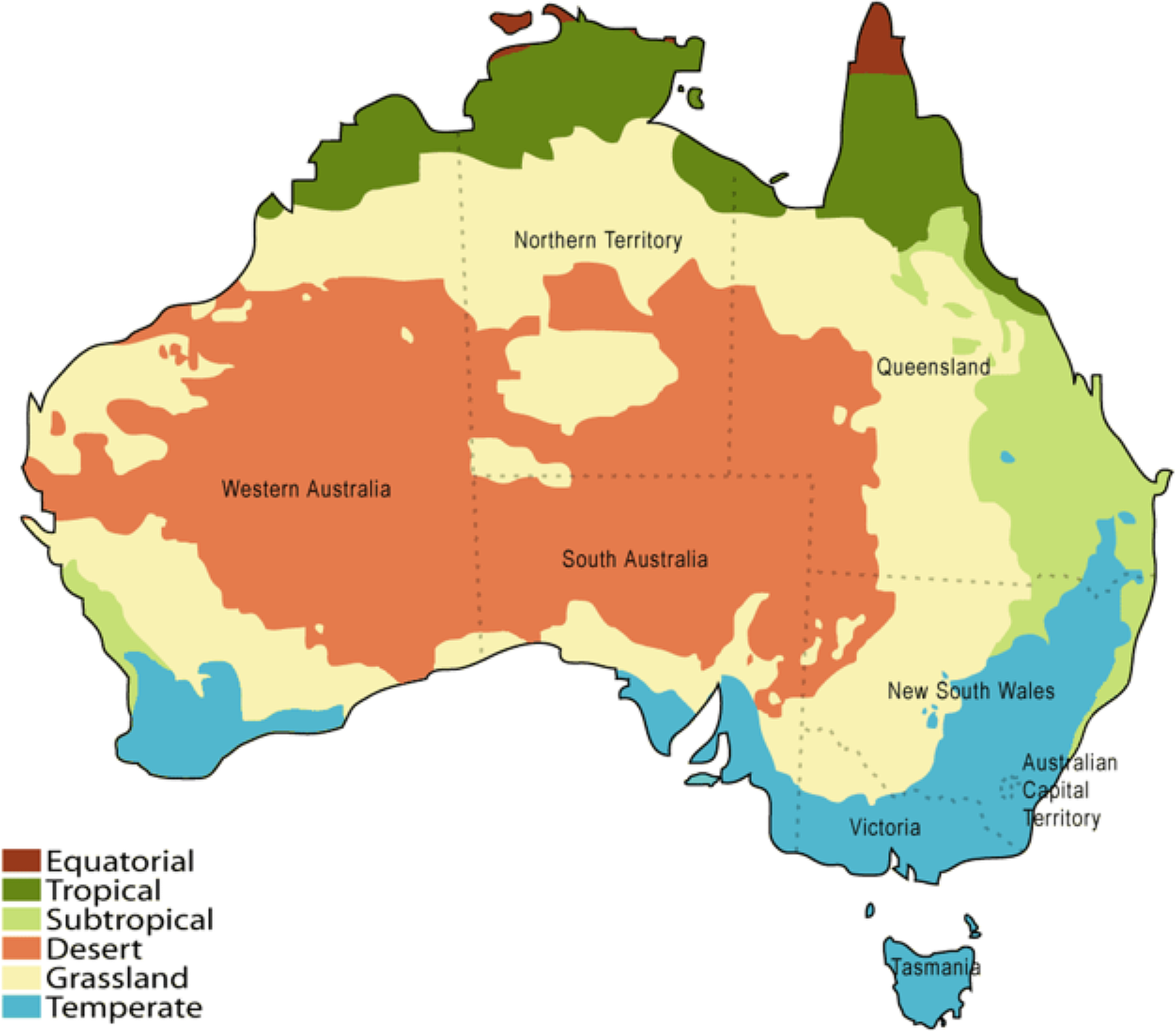
S. aureus was the commonest cause of bacteraemia in tropical Australia [17, 18, 20]. The annual incidence of S. aureus bacteraemia in tropical Australia ranged between 17 and 96 per 100,000 population during the period 2000 to 2019 according to the studies conducted in Northern Territory and Northern Queensland [16,17,18,19,20,21] (Table 1). The rates were lower in children which was around 10 to 20 cases per 100,000 population [22, 23]. High incidence of S. aureus bacteraemia was observed among the Indigenous patients compared to non-Indigenous [16, 19, 23, 31]. Many long-term studies conducted during 2000 to 2020 in tropical Australia revealed a decline in S. aureus bacteraemia [17, 20, 22]. This could be attributable to infection control measures in healthcare settings [20]. It is notable these findings run counter to the global trends. According to a systematic review, in the global setting, there were variable trends for S. aureus bacteraemia with no significant change in the incidence across the included countries from 2000 to 2020 [32].
Incidence rates of S. aureus bacteraemia in tropical Australia were found to be higher than that of the national rates. Annual incidence of S. aureus bacteraemia in Australia between 1999 and 2010 ranged from 11.2 to 35 per 100,000 population [31, 33], whereas the annual incidence of S. aureus bacteraemia in tropical Australia was as high as 96.6 per 100,000 population in some parts [17]. The latter study was conducted in the Northern Territory and described a high proportion of Indigenous people and numerous comorbidities.
Crude mortality rate of S. aureus bacteraemia in tropical Australia, ranged between 4 and 8% [16, 18]. Interestingly, a study conducted in Australia and New Zealand revealed a low mortality rate (7%) for Indigenous patients compared to non-Indigenous (17%) [31]. The probable explanation for this could be that Indigenous patients had a younger average age of acquisition of the infection [31].
MRSA Bacteraemia
The annual incidence of MRSA bacteraemia in tropical Australia ranged between 3.8 and 17 per 100,000 population within 2004 to 2015 [16, 18, 20,21,22] (Table 1). MRSA has different strains which can be differentiated based on resistance to non-methicillin antibiotics. Multiresistant MRSA (mrMRSA) exhibit resistance to multiple classes of antibiotics and are comparatively common in hospitals, whereas Non-multiresistant MRSA (nmMRSA) remain susceptible to some classes of antibiotics (cotrimoxazole, clindamycin and macrolides) and are comparatively common in the community.
Studies conducted in different tropical settings reported different trends of MRSA bacteraemia. The 10-year study conducted in Northern Queensland found that overall incidence of MRSA did not change significantly over the study period. However, mrMRSA significantly reduced during this period (P = 0.04) while nmMRSA increased, which was not statistically significant (P = 0.125) [20]. A paediatric study conducted in Northern Queensland from 2001 to 2010 revealed an increase in the number of MRSA bacteraemia during the study period [22].
Northern Australia, as noted by Murray et al. (2004), experienced a surge in community-onset MRSA bacteremia [21]. This increase in community-acquired MRSA infections has been noted throughout Australia. [33, 34]. A study conducted in 17 Australian hospitals revealed that 40% of the S. aureus bacteraemia episodes were hospital onset MRSA while 12% were of community onset [33]. Crowded living conditions, poor hygiene and heavy use of broad-spectrum antibiotics are proposed mechanisms by which there is increasing emergence of community acquired MRSA [35].
MRSA bacteraemia was found to be more prevalent among Indigenous people [19, 31]. Female sex and remote residence were significantly associated with resistant strains of MRSA compared to sensitive strains [16]. Mortality rates of MRSA ranged between 2% (MSSA) to 4.5% (MRSA) [16].
Group A Streptococcus (GAS) Bacteraemia
GAS bacteraemia is an invasive disease which frequently leads to life threatening consequences such as septicaemia and streptococcal toxic shock syndrome (STSS). Incidence of GAS bacteraemia among the general population in tropical Australia ranged between 7.45 and 20 per 100,000 population per year [17, 20, 24,25,26, 36] (Table 1). A high incidence rate for GAS bacteraemia was observed among Indigenous populations. Three large studies conducted in North Queensland and Northern Territory during 1996 to 2014 period revealed that the incidence among Indigenous population was 4–10 times higher compared to the total population incidence [24,25,26]. A paediatric study conducted in Northern Queensland from 2001 to 2010 revealed a relatively lower rate of incidence of GAS bacteraemia fluctuating between 0 and 7 per 100,000 population over the study period [22].
A significant rise in GAS bacteraemia was observed in Northern Territory during 1999 to 2019 period [17] while it was stable in Northern Queensland during 1996 to 2009 [36]. A steep rise in the reported incidence of invasive GAS (iGAS) disease across Australia was observed during 2018 to 2022 period from a large study [37]. This increase in reported case numbers could be due to increased case detection rate as a result of iGAS becoming a nationally notifiable disease during the period 2005 to 2021 in Australia [38]. Increasing incidence rates were observed in global literature as well [24, 39]. Likewise, Indigenous communities were at increased risk of infection with GAS globally [40, 41]. This can be explained by the strong relation of this pathogen to the social determinants of health, where Indigenous communities experience more socioeconomic disadvantages comparatively [26, 42].
Having chronic diseases like diabetes, chronic kidney disease, cardiac diseases and receiving dialysis were risk factors for GAS bacteraemia [26]. According to literature from tropical Australia, crude mortality rate of GAS bacteraemia ranged between 5.6 and 13.8% [24,25,26, 36]. Proportion of cases requiring ICU admissions varied from 15.0 to 23.6% while STSS was reported from 6.6 to 16.3% of these patients [25, 26]. Antimicrobial resistance was present in 19.2%, most commonly to tetracycline [26].
Group B Streptococcus (GBS) Bacteraemia
Group B Streptococcus frequently causes morbidity and mortality among vulnerable populations, such as pregnant mothers, newborns, and the elderly [36]. GBS bacteraemia can lead to sepsis, pneumonia and meningitis. Studies conducted in Northern Queensland from 1996 to 2020 revealed a rise in incidence from 4.3 to 11.4 per 100,000 per year [20, 27, 36]. The incidence of GBS bacteraemia was about 2.5 times higher among the Indigenous population compared to non-Indigenous population [27]. However, another high-risk group was the non-Indigenous older females [36]. One important observation throughout the studies was that GBS bacteraemia was deviating from being predominantly a neonatal and maternal infection to become a non-neonatal and non-pregnant infection [27, 36]. This change was observed in studies conducted globally [43,44,45,46,47]. Another interesting observation was that as age advanced, a switch from Indigenous cases to non-indigenous became apparent [27].
Presence of comorbidities was a risk factor for GBS bacteraemia [27]. Crude mortality rate was 3.6% [36] with an increased risk among males and immunosuppressed patients [27].
Streptococcus pneumoniae Bacteraemia
S. pneumoniae bacteraemia was found to be the commonest bacteraemia among children in tropical Australia [22]. Three recently conducted studies in tropical Australia between 2000 and 2019 revealed a reduction in reported S. pneumoniae bacteraemia [17, 20, 22] (Table 1). This decrease can largely be attributed to the successful pneumococcal vaccination programs in tropical Australia [20]. There was insufficient research on S. pneumoniae bacteraemia from tropical Australia to describe the associated risk factors and mortality.
Escherichia coli and Klebsiella pneumoniae Bacteraemia
E. coli was found to be the commonest gram-negative organism causing bacteraemia in Australian tropical regions [17, 18, 20]. The incidence of E. coli bacteraemia in the general population ranged between 19 and 48 per 100,000 per year during 2004 to 2020 in tropical Australia [17, 18, 20, 22]. There was conflicting evidence on trends of E. coli bacteraemia reported from tropical Australia. One study reported a 2.5 fold increase in the incidence of E. coli bacteraemia from 1999 to 2019 surpassing the number of S. aureus bacteraemia at the end of the study period [17]. But a more stable trend was observed in the paediatric population according to a study conducted in Northern Queensland from 2001 to 2010 [22]. However, an increas in incidence was observed globally for E. coli bacteraemia especially in European countries [48, 49].
E. coli was noted to have a decrease in its susceptibility to gentamicin over the study period [20]. Crude mortality rate of E. coli bacteraemia was found to be around 10% [18].
Klebsiella spp. were found to be frequent pathogens causing gram negative bacteraemia in tropical Australia ranging between 3 and 18 per 100,000 per year during 1999 to 2019 [17, 18, 20, 22] (Table 1). A significant increase in the incidence of Klebsiella bacteraemia was reported from Northern Territory [17].
Burkholderia pseudomallei Bacteraemia
B. pseudomallei is an organism predominantly found in tropical and subtropical regions causing melioidosis. This has a strong seasonal preference, occurring in wet season [50]. Bacteraemia is a common consequence of melioidosis. In Northern Queensland and Northern Territory of Australia the incidence of B. pseudomallei bacteraemia ranged between 3 and 19 per 100,000 per year during 1998 to 2020 with an increase in incidence over that period [17, 18, 20, 28,29,


留言 (0)