Data collection and definitions
This is an observational cohort study performed at the University Hospital of Geneva (HUG), a Swiss academic tertiary medical care center. The STROBE guidelines were followed to improve the quality of the study [15].
Data from all adult patients (aged ≥ 18 years) treated for SE between November 1st, 2015 and December 31st, 2023 were retrospectively identified from a SE registry retrospectively collected to October 2021, and prospectively collected from November 2021 to 2023.
Data were collected and managed with the password encrypted online browser-based, metadata-driven database organizer REDCAP (Research Electronic Data Capture) [16].
Patients with SE following cardiorespiratory arrest and patients without blood gas analysis (BGA) during the first 24 h of SE were excluded.
The following features were retrieved: patients’ age, sex, comorbidities, SE etiology, semiology, and duration. SE types were defined as recommended by the International League Against Epilepsy (ILAE) [1]. SE etiology was defined as acute symptomatic, remote symptomatic, progressive symptomatic, and unknown [1]. SE etiology was categorized as potential non-fatal and fatal, following previous reports [17].
Charlson Comorbidity Index (CCI, range 0–37) and the Status Epilepticus Severity Score (STESS, range 0–6) were calculated to quantify comorbidity burden and illness severity, respectively [18,19,20].
Sepsis has been defined in the presence of established infection together with organ dysfunction, represented by an increase in the Sequential (sepsis-related) Organ Failure Assessment (SOFA) score of 2 points or more [21, 22].
SE duration was defined as the period between SE diagnosis and the clinical and/or EEG evidence of seizure termination, as described elsewhere [23].
The Glasgow Outcome Scale (GOS, range 1–5) was used to assess outcome at discharge, dichotomized as follows: bad outcome—GOS of 1 to 3; good outcome—GOS of 4 to 5 [24].
Values of pH, partial pressure of carbon dioxide (PaCO2) and bicarbonate (HCO3–) from BGA during the first 24 h of SE were gathered. The following laboratory data within the first 24 h of SE were also collected: serum albumin [g/L], serum creatinine [umol/L], serum phosphate [umol/L], serum bilirubin [umol/L], serum urea [umol/L], serum sodium [mmol/L], and serum potassium [mmol/L].
Values obtained beyond 24 h from SE onset were excluded. For patients with multiple laboratory values within the first 24 h, only the first assessment was considered.
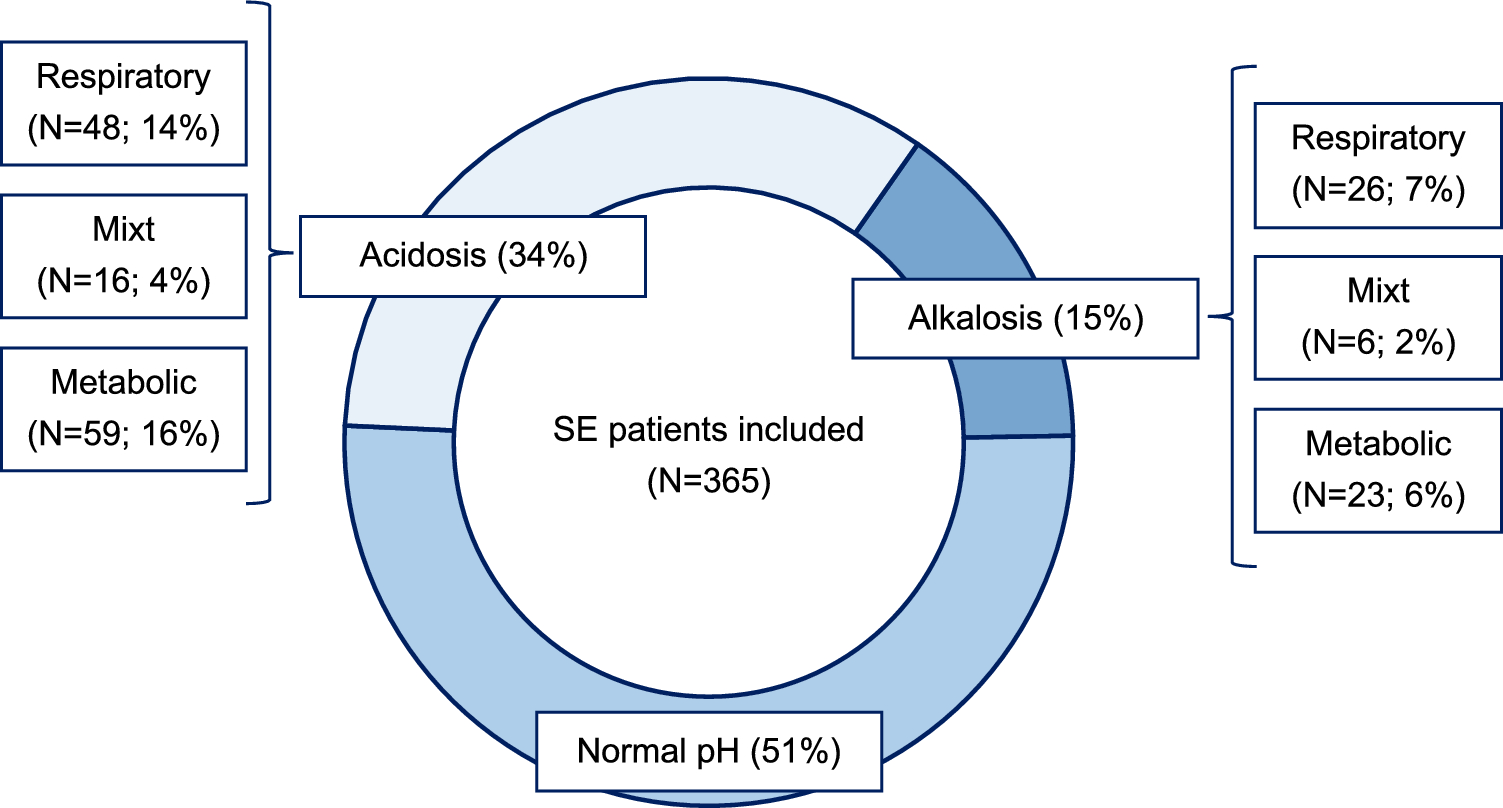
According to the Henderson–Hasselbalch equation [25], the following acid–base disturbance categories were defined: acidosis (either Respiratory [pH < 7.35, PaCo2 > 45 mmHg], metabolic [pH < 7.35, HCO3 < 22 mmol/L] or mixt [pH < 7.35, PaCo2 > 45 mmHg, HCO3 < 22 mmol/L]), normal pH (pH 7.35–7.45) and alkalosis (either respiratory [pH > 7.45, PaCo2 < 35 mmHg], metabolic [pH > 7.45, HCO3 > 26 mmol/L] or mixt [pH > 7.45, PaCo2 < 35 mmHg, HCO3 > 26 mmol/L])[26, 27].
In addition, to better identify predominant metabolic alkalosis in patients with complex acid–base disorders, we used the Stewart approach, which posits that the body’s pH is primarily determined by the difference in charge between strong ions and weak acids. According to this method, the presence of metabolic alkalosis is indicated by an effective Strong Ion Difference (SIDe) > 40 mEq/L, and/or serum hypoalbuminemia (< 35 g/L). We defined metabolic alkalosis as the predominant acid–base disturbances in the presence of pH > 7.45, SID > 40 mE/L and/or hypoalbuminemia [28, 29].
Outcomes
Primary outcomes were the relationships among acid–base categories and in-hospital mortality, GOS at discharge [24] and return to baseline premorbid neurologic function at discharge.
Secondary outcome was the distribution of acid–base disturbances according to the Henderson–Hasselbalch equation in the SE patients.
Statistics
Univariable comparisons were performed by the χ2 test for categorical variables. For continuous variables, the Shapiro–Wilk test was used to distinguish between normally and not normally distributed variables.
We assessed relationship among acid–base disturbances according to the Henderson–Hasselbalch equation and primary outcomes first through univariate analyses and then through a binomial regression model considering unbalanced univariate results and variables potentially related to outcomes (age, CCI, SE semeiology, SE potentially fatal etiology, SE duration, STESS, and reliance of invasive therapies).
Then we examined the association between predominant metabolic alkalosis according to the Stewart approach and primary outcomes using both univariate analyses and a binomial regression model.
We assessed laboratory variables associated with the presence of metabolic alkalosis according to according to the Henderson–Hasselbalch equation and the Stewart approach through univariate analysis.
Finally, given the known correlation between sepsis and acid–base unbalance, we performed a subgroup analysis considering only patients with sepsis and evaluating acid–base distribution in this population together with correlation with outcome.
All analyses were performed utilizing the Jamovi software (2.3.21.0 Version).





留言 (0)