Ethics approval
This study was designed as a retrospective study in line with the principles of the Declaration of Helsinki and approved by the Independent Ethics Committee. All participants provided informed consent for inclusion before their participation in the study. And this work has been reported in line with the STROCSS criteria [9].
Patient selection
The initial 125 cases of bDAA and mDAA THA, conducted by the same surgeon and adhering to the inclusion and exclusion criteria, were retrospectively enrolled from September 2020 to February 2022.
Inclusion criteria included: (i) patients underwent primary THA via bDAA, or mDAA; and (ii) patients diagnosed with avascular necrosis of the femoral head, femoral neck fracture, congenital hip dysplasia (Crowe type 1, 2), osteoarthritis, rheumatoid arthritis, or ankylosing spondylitis.
Exclusion criteria included: (i) patients with other hip fractures other than the femoral neck; (ii) patients undergoing revision hip arthroplasty; (iii) severe congenital hip dysplasia (Crowe type 3, 4); (iv) combined with serious diseases affecting postoperative rehabilitation exercise, such as severe knee joint disease, spinal disease, etc.; and (v) incomplete follow-up data of patients.
Preoperative characteristics including age, gender, BMI, ASA classification, follow-up time and predicted blood volume were collected. The predicted blood volume for each patient was conducted using the method described by Nadler [10]. This method calculates blood volume based on the patient's height and weight.
Surgical technique
All surgical procedures were performed by the same surgeon who had not previously encountered bDAA. The surgeon had prior extensive experience with completing posterior and lateral approaches.
Anesthesia and position
The patients were positioned supine, with their pubic symphysis aligned with the fold of the operating table. A “cocktail mixture” (composed of 150 mg of ropivacaine, 1/2 vial of adrenaline 1:10,000, and diluted with physiological saline to 100 ml) of local infiltration analgesia was administered prior to making the skin incision.
Approach and exposure
The mDAA approach has been elucidated in a previous study [8]. An incision measuring approximately 5 ~ 6 cm in length was made in the lateral groin crease. To minimize lateral cutaneous femoral nerve (LFCN) injury, the length of the incision should constitute two-thirds of the total length along the lateral aspect of the anterior superior iliac spine line. Proceed by making a horizontal cut through the skin and subcutaneous layer, followed by a vertical incision through the deep fascial tissue. Upon identifying the interval between the tensor fasciae latae and the sartorius muscle, access to the Hueter interval was established. The subcutaneous tissue on the medial side of the Hueter gap was separated and retracted medially to protect the LFCN. Through the Hueter gap, the lateral femoral circumflex artery was identified and dissected. The articular capsule was incised to form a flap. A Hohmann retractor was used to protect the LFCN. Employing a two-knife technique, the femoral neck was excised to ensure the femoral head could be removed separately through the minimally invasive incision.
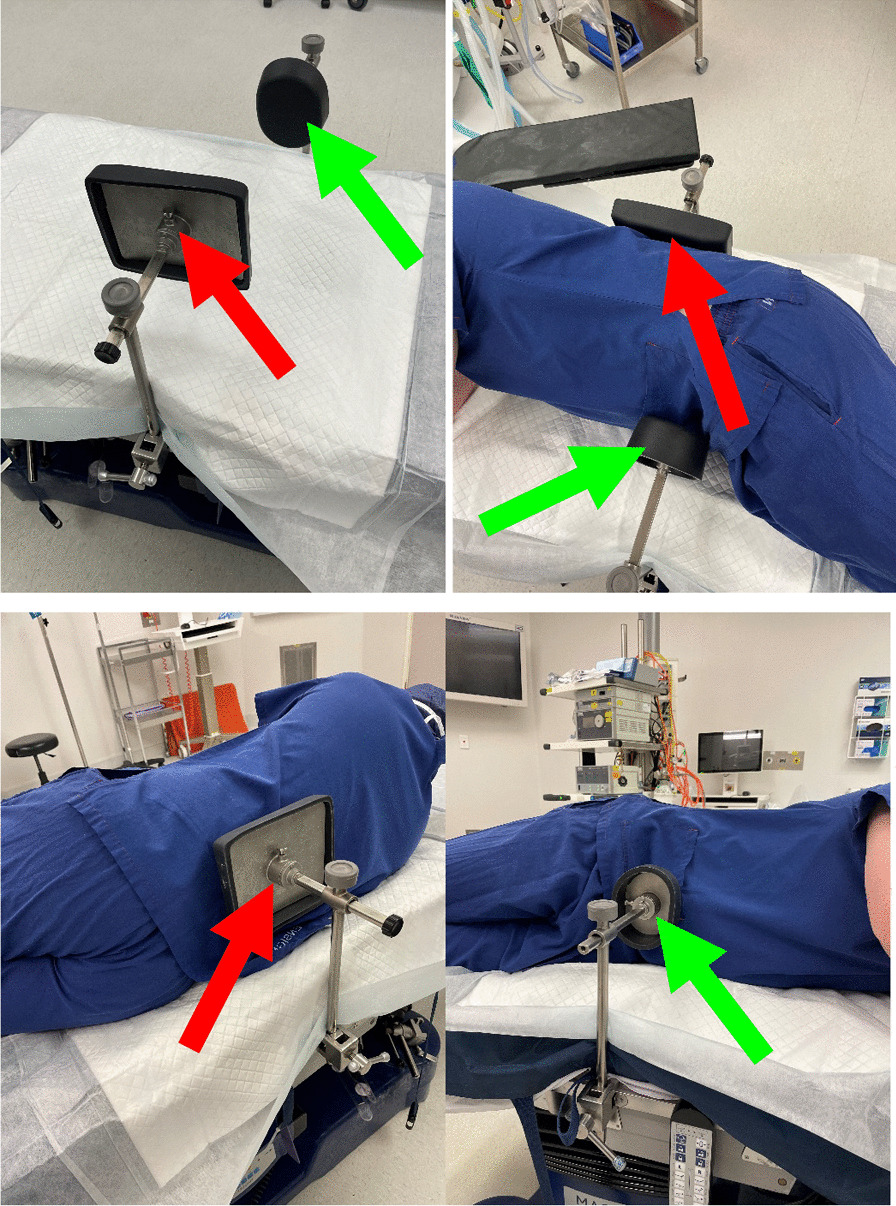
Using a “finger-touch” technique, a percutaneously-assisted channel of approximately 1 cm was placed at a muscle interval about 10 cm distal to the primary incision. Selectively placed a commonly used disposable laparoscopic trocar at the percutaneously-assisted channel. Preparation of the acetabulum was performed under endoscopy. The acetabular reamer was placed through the main incision, and the handle was introduced through the percutaneous access. Once assembled, it was used to ream the acetabulum to the preoperatively planned depth. After placing the acetabular component through the main incision and adjusting it to the proper position, an impactor was placed through the percutaneously-assisted channel to impact the prosthesis until it was stabilized.
The operating table was adjusted to hyperextend the hip joint by approximately 30–40°. A lift-top tractor (Chinese National Patent, Patent Number: ZL201821970909.X) was utilized to elevate the proximal femur. Subsequently, the medullary cavity was reamed based on preoperative measurements. Following assessment of lower limb length, prosthesis stability, joint mobility, and impingement phenomenon, the femoral stem prosthesis and femoral head were inserted.
In the bDAA group, the incision length is approximately 6–8 cm, located 2 cm distal to the anterior superior iliac spine. Meanwhile, percutaneously-assisted channels are not used during the surgery.
Perioperative care
All patients received the same standardized perioperative treatment regimen. Antibiotics and tranexamic acid were administered via intravenous infusion preoperatively. Patients promptly commenced a standardized multimodal analgesia regimen postoperatively. Early mobilization with weight-bearing exercises was encouraged on the day of the operation. Oral administration of rivaroxaban was routinely recommended for a duration of 5 weeks postoperatively.
Outcomes
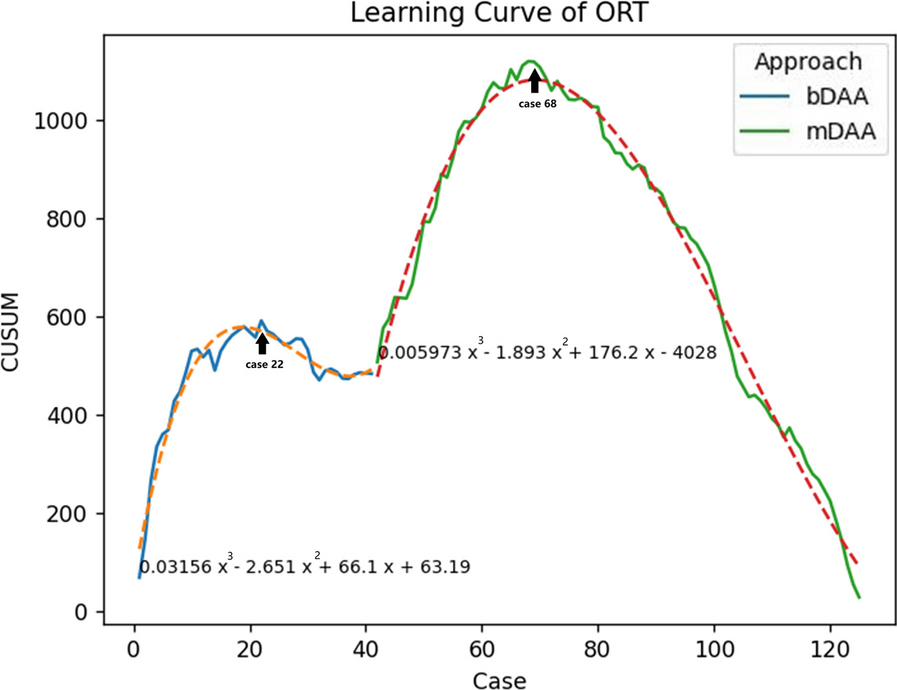
All patients were followed-up at 2 weeks, 6 weeks, 6 months and 12 months. The followed-up results were obtained from the prospectively established clinical records database. The primary study outcome was the operating room time (ORT), defined as the total duration in minutes from entering to exiting the operating room for it has been proved to be the most difficult outcome to improve. Secondary outcomes include perioperative outcomes and postoperative complications. Perioperative outcomes encompass the length of incision (LOI), reduction of hemoglobin in grams per deciliter, transfusion requirements, and length of stay (LOS). Postoperative complications include Harris Hip Scores at 12 months (HHS), wound-healing problems (wound ooze and delayed wound healing), venous thrombo embolism (VTE), LFCN dysesthesia (defined as numbness in the region innervated by LFCN), infection, revision, periprosthetic fracture, and dislocation.
Statistical analysis
For normally distributed continuous variables, data were presented as means and standard deviations and intergroup differences were assessed for significance using Student t-test. Otherwise, the data were presented as median and quartiles, and were compared using the Mann–Whitney U test. χ2 tests were applied for categorical variables. The learning curve was analysed using the cumulative sum method (CUSUM). This involved employing cumulative sums to assess the ORT across a sequential series of operations, aimed at determining proficiency in surgical performance and if the learning curve was overcome. Fitting curves based on the increase in cases according to ORT, representing estimated ORT. Generalized linear modeling was used to model ORT of the mDAA group. Multivariable analysis was performed in a stepwise analysis and presented as odds ratios (ORs) with 95% confidence intervals, estimated probability and coefficients to ORT of the mDAA group. All statistical tests were 2-sided, and differences were considered significant when P was less than 0.05. Statistical analyses were performed using Python 3.12 and SPSS 22.0.






留言 (0)