
記住我





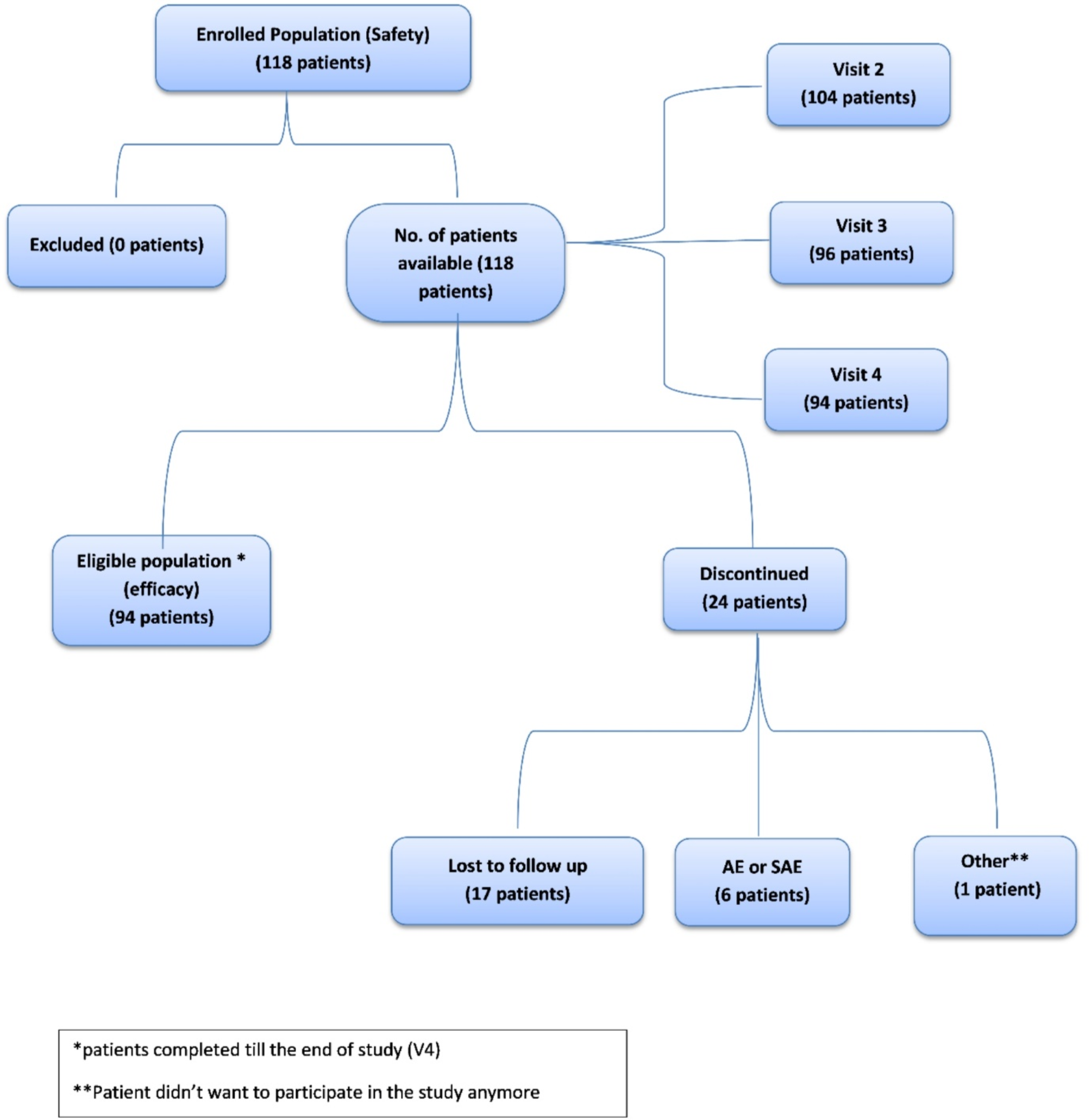



A total of 425 adolescents and young adults (13–25 years) completed the 6-week, double-blind, placebo-controlled trial, of whom 306 patients (72%) provided informed consent and continued the 12-month extension study, including 208 patients who were initially randomized to double-blind lurasidone (who continued on lurasidone in the extension study) and 98 patients who were randomized to double-blind placebo (who were switched to lurasidone at entry into the extension study). Switching was accomplished while maintaining the double-blind nature of the initial 6-week trial.
Demographic and clinical characteristics at the extension phase baseline were similar for patients receiving lurasidone or placebo during the initial core study, except for greater severity in the core placebo group according to the PANSS total score (79.2 vs. 72.4) and CGI-Severity score (4.2 vs. 3.7; Table 1).
Table 1 Baseline characteristics by treatment assignment during the initial randomized, double-blind, 6-week study (safety population)The following concomitant medications were used during the course of the pooled extension studies: anxiolytics (71/306; 23.2%), benzatropine or other anticholinergic medication (28/306; 9.2%), propranolol (6/306; 2.0%), and sedative/hypnotics (21/306; 6.9%).
A total of 208 patients (68.0%) completed 12 months of treatment with lurasidone, 68.3% in the core lurasidone group and 67.3% in the core placebo group. The Kaplan‒Meier estimates of the median [95% CI] time to discontinuation during the extension phase were similar in both groups: 375 [375, –] days vs. 371 [368, –] days, respectively. The Kaplan‒Meier estimate of the probability of discontinuation was 0.30 for both groups. The reasons for discontinuation in the extension phase (by original core lurasidone vs. placebo assignment) were as follows: lack of efficacy (5.3% vs. 3.1%), adverse events (7.7% vs. 9.2%), withdrawal of consent (9.6% vs. 13.3%), loss to follow-up (2.9% vs. 2.0%), and miscellaneous reasons (6.2% vs. 5.1%).
EffectivenessFor the PANSS total score, the mean (95% CI) observed changes from the extension phase baseline for the overall safety sample were − 9.5 (− 11.0, − 8.0) at Month 3, − 11.8 (− 13.5, − 10.0) at Month 6, − 13.7 (− 15.6, − 11.8) at Month 9, − 15.3 (− 17.3, − 13.3) at Month 12, and − 10.5 (− 12.6, − 8.5) at the LOCF endpoint. For the subgroup treated with lurasidone in both the core and extension phases, the mean (95% CI) change from the core baseline was – 22.2 (− 24.3, − 20.0) at the acute endpoint (Week 6), and the mean (95% CI) changes from the extension phase baseline were − 7.5 (− 9.1, − 5.9) at Month 3, − 9.9 (− 11.8, − 8.0) at Month 6, − 12.0 (− 14.1, − 9.8) at Month 9, − 13.8 (− 16.1, − 11.4) at Month 12, and − 8.8 (− 11.2, − 6.3) at the LOCF endpoint.
Figure 1A shows the mean change from the core baseline in the extension study (by original core lurasidone vs. placebo assignment). For patients switching from core placebo to lurasidone, the reduction in the PANSS total score was approximately “caught up” by Month 3 of the extension phase, with the improvement achieved in the core lurasidone group. For both groups combined, − 17.3/− 33.8 (51.2%) of the reduction in the PANSS total score (from core-baseline to month 12) occurred during the 12-month extension phase. For the subgroup treated with lurasidone in both the core and extension phases, − 17.3/− 33.8 (51.2%) of the reduction in the PANSS total score (from core-baseline to month 12) occurred during the 12-month extension phase.
The proportion of improvement from core-baseline to month 12 that occurred during the extension phase was 42.5% for the PANSS-positive subscale score, 42.9% for the negative subscale score, and 44.9% for the general psychopathology score (Fig. 1B).
Fig. 1
Effectiveness Measures. A Mean change in the PANSS total score from the double-blind baseline (by original treatment assignment in the double-blind study). B Mean Changes in PANSS Subscale Scores from Double-blind and Extension Phase Baselines
On the CGI-Severity score, the mean (95% CI) observed changes from the extension baseline for the overall safety sample were − 0.6 (− 0.7, − 0.5) at Month 3, − 0.8 (− 1.0, − 0.7) at Month 6, − 1.0 (− 1.1,− 0.8) at Month 9, − 1.0 (− 1.2, − 0.9) at Month 12, and − 0.7 (− 0.8, − 0.6) at the LOCF endpoint. Figure 2 shows the mean change from the core baseline in the extension study (by original core lurasidone vs. placebo assignment). For patients who switched from core placebo to lurasidone, this reduction in the global CGI-S score approached that of Month 3 but never quite “caught up”, with the improvement achieved in the core lurasidone group.
Fig. 2
Mean change from double-blind baseline in CGI severity score (by original treatment assignment in the double-blind study)
For the overall safety sample, treatment response rates, based on a stringent reduction of ≥ 30% in the PANSS total score, showed an incremental increase during the 12-month course of treatment with lurasidone (Fig. 3). were 94.1% and 92.5% at week 26 (observed case) and 74.0% and 73.1% at the LOCF endpoint, respectively, and the response rates (≥ 50% reduction in PANSS) were 76.5% and 67.9% at week 26 (observed case) and 54.5% and 48.7% at the LOCF endpoint, respectively. The remission rates, based on the Andreasen criteria (36) and requiring 6 months of continuous symptom reduction, were 53.7% at Month 6, 57.7% at Month 9, and 60.4% at Month 12 (OC).
Fig. 3
Response Rates (During 12 Months of Extension Phase Treatment) and Sustained Remission Rates (During 6 Months of Extension Phase Treatment)
Among the 139 patients who met the responder criteria at Month 3, the Kaplan–Meier estimate of the probability of relapse at the end of the 12-month extension treatment period was 0.08. Among the 130 patients who met the Andreasen 6-month remission criteria, the Kaplan–Meier estimate of the probability of relapse at the end of the 12-month extension treatment period was 0.10.
SafetyIn the extension study, the overall incidence of AEs was 71.6%, resulting in an 8.2% discontinuation rate for AEs among all extension-phase patients. Twelve AEs were reported with an incidence ≥ 5%: headache (17.6%), anxiety (11.4%), schizophrenia (9.8%), nausea (9.8%), agitation (7.5%), agitation (7.2%), somnolence (6.9%), insomnia (5.9%), dizziness (5.6%), vomiting (5.6%), nasopharyngitis (5.2%), and weight increase (5.2%). Only one AE (weight increase) was meaningfully greater (≥ 5%) in the core placebo group than in the core lurasidone group (9.2% vs. 3.4%).
The mean (SD) changes from the core baseline in weight and BMI during 12 months of extension treatment with lurasidone were + 2.5 (5.1) kg and + 0.5 (1.6) kg/m2, respectively.
The effect of 12 months of treatment with lurasidone revealed small median changes in metabolic laboratory parameters, including total cholesterol (− 3.0 mg/dL), LDL cholesterol (− 1.0 mg/dL), triglycerides (− 1.0 mg/dL), and glucose (+ 1.0 mg/dL), from the core baseline (Fig. 4). Treatment with lurasidone had minimal effect on median serum prolactin levels in both females (+ 1.3 ng/mL) and males (0.0 ng/mL).
Fig. 4
Key laboratory values: median change from double-blind baseline to month 12
留言 (0)