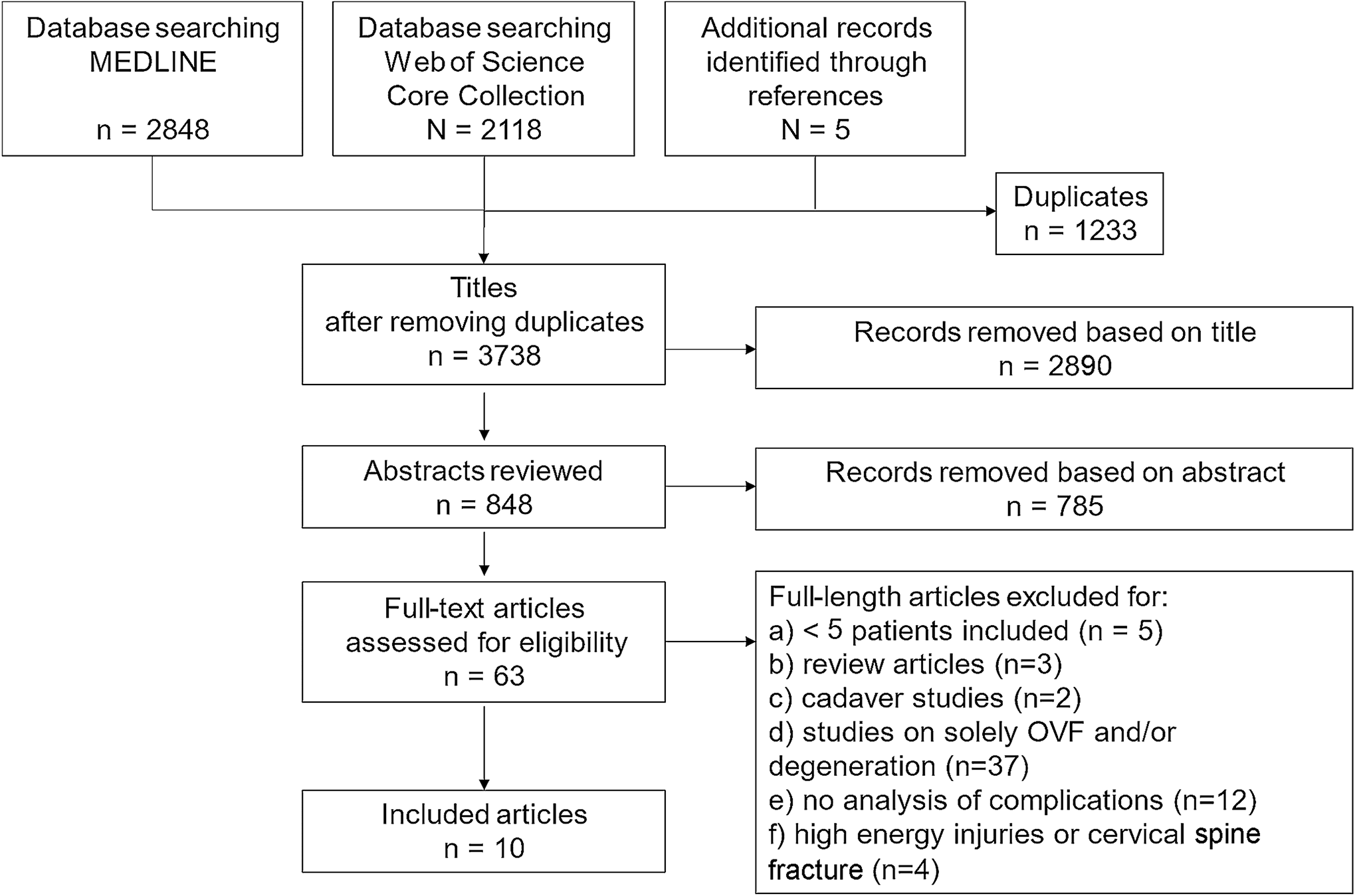
Study selection
Ten studies met the inclusion criteria (Tables 1 and 2). The publication dates ranged from 1991 to 2022. Common reasons for exclusion were no primary data, absence of or missing information on osteoporosis or degeneration, no occurrence of spine fracture, and missing information on complications (Fig. 1).
Articles were divided into two groups. Five studies involved patients who were treated for OVFs and had coexisting degenerative spinal conditions. In the remaining five studies, OVFs were treated following surgical treatment for degenerative spinal conditions. Tables 1 and 2 present a tabulated summary of the manuscripts and their relevant results. Table 3 summarizes the treatments and complications.
Table 1 Included studies of group 1: patients who were treated for OVF and had coexisting degenerative spine conditionsTable 2 Included studies of group 2: occurrence of OVF following surgical treatment for degenerative spine conditionsTable 3 Described treatments and listed complicationsPatients who were treated for OVF and had coexisting degenerative spine conditions
This group included one case series (n = 8), two retrospective cohort studies, one prospective single-center study and one prospective, multicenter study (Table 1).
Three studies found more complications in patients with acute (proven by MRI) OVFs if there was underlying degeneration.
Sabo et al. [11] described a case series of eight women > 75 years who underwent surgical treatment for OVFs (vertebroplasty or kyphoplasty) and to correct a lumbar scoliotic curve between 6–50°. The measurement of osteoporosis was not further elaborated upon. The presence of lumbar scoliosis led to OVFs and was associated with subsequent OVFs in the following months (n = 8/8), sacral insufficiency fractures (n = 3/8) and other fractures (n = 3/8). No threshold for the severity of scoliosis was defined, and the authors reported that 38% (n = 3) of patients had scoliosis > 20°. Based on their findings, the authors recommended medication for osteoporosis, early treatment for fractures affecting the coronal profile, and augmentation of adjacent vertebrae.
Oishi et al. [12] identified coexisting degenerative spondylolisthesis at the OVF level as a risk factor for the occurrence of neurological deficits. Patients with neurological deficits had a significantly higher frequency of coexisting degenerative spondylolisthesis at the affected disc level than those without neurological deficits (50% [11/22] vs. 13%, [11/82], p < 0,005) [12]. Coexisting degeneration and neurological symptoms depended on the signal intensity in the T1W MR images. The bone mineral density (BMD) of the hip was measured using dual-energy X-ray absorptiometry (DXA). OVFs indicated by total low intensity might have had increased bone fragility compared to those with OVFs indicated by superior/inferior low intensity. However, OVFs indicated by superior/inferior low intensity on T1W MR images was more often associated with coexisting degenerative spondylolisthesis than OVFs indicated by total low intensity (26.3% [6/28] vs. 21.4% [15/57]) and resulted more often in the occurrence of neurological symptoms.
In a single-center prospective study, Estublier et al. [4] analyzed the relationship between disc degeneration and acute fragility fractures in men. Disc degeneration was defined using a four-point scale based on the severity of disc space narrowing. Of the 765 men, 64 had a preexisting OVF. The BMD of the hip and the spine were measured using DXA.
In 659 men with follow-up radiographs, 28 incident vertebral fractures occurred in 27 men over 7.5 years. They concluded that severe disc degeneration is accompanied by higher spinal bone mineral density and an increased risk of vertebral fractures.
In contrast, in a multicenter prospective study, Rahmani et al. [13] described that fracturing of the endplate and less disc degeneration were risk factors for non-union of OVFs. They classified preexisting disc degeneration into eight groups based on the modified Pfirrmann grading system, considering nucleus signal intensity, distinction between the inner and outer fibers of the annulus, and posterior aspects of disc and disc height. DXA has been used to measure the BMD of the hip. Existing disc degeneration appears to be associated with higher BMD. However, the relationship between BMD, degeneration, and OVFs has not been further analyzed. The patients were treated conservatively with corsets (96%) and teriparatide (14%). Delayed union at the 6-month follow-up could be seen in 27 cases (19%). They discussed a higher motion level of a healthier disc as a risk factor for poor fracture healing.
Ross et al. [14] found no association between preexisting degeneration and OVFs. Of the 897 women, 61 had at least one preexisting OVF. Twenty-four (6.6%) patients sustained subsequent fractures during an average follow-up of 4.7 years. Spinal degeneration (osteoarthritis, spondylolisthesis, disc degeneration, and scoliosis), whether absent or present, did not have a significant influence. Notably, Ross et al. [14] solely investigated radiographs and not magnetic resonance images. They found that poor bone mass and the number of vertebral fractures were risk factors for subsequent fractures. A difference of two standard deviations (SD) in bone mass led to a rate ratio of 3-4.4 for a new OVF. Therefore, the authors recommended a systemic treatment for osteoporosis.
Occurrence of OVF following surgical treatment for degenerative spine conditions
This group included five retrospective cohort studies (Table 2). The studies involved patients with degenerative spine diseases and OVF and listed complications without investigating further interactions or conclusions.
Hayashi et al. [15] retrospectively analyzed the outcome of posterior lumbar interbody fusion (PLIF) for spinal canal stenosis, spondylolisthesis or degenerative lumbar scoliosis. Twelve of 96 (12.5%) patients had preexisting acute OVFs, and 18 (19%) patients presented with a newly identified postoperative OVF.
The method for measuring osteoporosis was not further elaborated upon. Overall, perioperative complications (anemia, cardiopulmonary, gastrointestinal or urinary tract infections) were identified in 16 patients (17%), surgery-specific complications (dural tear, hematoma, neurologic deficit, infection, implant failure, non-union, and adjacent segmental degeneration) occurred in 22 patients (23%), major complications (blood transfusion, additional antibiotics, treatment by another department) were noted in 11 patients (11.5%), and revision surgery was required in seven patients (7%). Liao and Chen [16] found significantly more preoperative OVFs (10.5% [4/38] vs. 2.6% [1/38]) and postoperative OVFs (13.2% [5/38] vs. 2.6% [1/38]) in patients older than 80 years after instrumented surgery for degenerative lumbar spondylolisthesis. In the group of patients aged ≥ 80 years, five postoperative complications were described: implant loosening (1 case), pneumonia (1 case), urinary tract infection (1 case) and wound infections (2 cases). The description of how osteoporosis was measured and the exact timing of the OVFs lack further detail.
In a retrospective study, Yang et al. [17] investigated the treatment options for urgent adjacent OVFs occurring after lumbar instrumented fusion for degenerative diseases in 23 patients. The BMD of the spine was measured using DXA. The BMD at the cranial level to fusion decreased time-dependent. All fractures were treated with percutaneous vertebroplasty. In addition to cement leakage in four patients, no surgery-related complications were reported. Two patients had new fractures within nine months: one was treated conservatively, and the other underwent vertebroplasty.
Kim et al. [18] retrospectively reviewed the data of 201 patients who underwent instrumented arthrodesis for degenerative lumbar disorders. Twenty-five patients suffered a subsequent OVF, which was associated with an aggravation of back pain. DXA has been utilized to measure the hip’s BMD, revealing a negative correlation with back pain. Lee et al. [19] compared the efficacy of non-operative treatment in comparison with decompression surgery in patients with lumbar spinal stenosis in a retrospective study. In the conservative group, 14/36 (39%) patients had a preexisting OVF, and 17/59 (29%) had a preexisting OVF in the surgery group. Preexisting OVFs did not influence the choice of treatment. The surgery group showed a greater decrease in the risk of falling, which did not correlate with the existing OVFs. The measurement of osteoporosis and the exact timing of the OVFs were not further expounded upon.





留言 (0)