Detection of PD-L1 expression in tissuesIHC
IHC is the main method for detecting PD-L1 expression. Thin slices of lung cancer tissue stained with specific PD-L1 antibodies were used to visualize PD-L1 expression under a microscope. To date, the detection of PD-L1 expression using IHC relies on four primary antibodies: Dako PD-L1 IHC 22C3 pharmDx and Dako PD-L1 IHC 28–8 pharmDx from Agilent Technologies; the VennTANA PD-L1 (SP142) and VennTANA PD-L1 (SP263) assays from Roche.
PD-L1 IHC results are typically reported as the percentage of tumor cells or immune cells that express PD-L1 at a specific intensity, which in turn reflects the response to ICIs. 22C3 and 28–8 correspond to the Dako diagnostic platform. The positive standard of the former stipulates ≥ 1% tumor cells. The staining of tumor cells was positive, ≥ 50% of tumor cells were strongly positive, and ≥ 1% of tumor cells were positive for the latter marker. SP142 and SP263 correspond to the Ventana diagnostic platform. The positive standard for the former is ≥ 10% tumor and/or tumor-infiltrating immune cell staining, and that for the latter is staining ≥ 25% tumor cells. Typically, at least 100 tumor cells are required to determine TPS.
Immunohistochemistry is widely used for PD-L1 detection because of its efficiency and stability. Notably, immunohistochemistry detection may yield false positives. This may be due to confusion between PD-L1-positive lymphocytes and histiocytes interspersed with PD-L1-negative tumor cells. In addition, granular cytoplasmic staining in nonmembranous malignancies may also be incorrectly interpreted as positive [12]. Currently, there is no gold standard for assessing the expression levels of PD-L1 in tumors and the TME. Further improvements in immunohistochemistry and the development of other PD-L1 detection technologies are still needed. In addition, since PD-L1 is partially expressed in tumor cells as well as in normal epithelial cells and lymphocytes, to improve the accuracy and resolution of staining results, multiplex immunohistochemical staining techniques can be utilized. These involve simultaneous labeling of antibodies against immune cells along with PD-L1 antibodies. This approach is highly important for assessing the status of the tumor immune environment and predicting the efficacy of immune therapy.
Immunofluorescence (IF) has been applied in the field of PD-L1 detection in recent years [13]. The principle of IF is similar to that of IHC. During this process, the antibodies are first labeled with fluorescein, and then the labeled antibody is bound to the corresponding antigen. Fluorescence microscopy was then used to determine the location of the antigen. Multiplex immunofluorescence (mIF) staining can quickly and reproducibly identify multiple molecular markers in the tumor microenvironment. Yaseen et al. confirmed that mIF has greater detection accuracy than does IHC or IF, which demonstrates its potential in clinical practice [14].
Glycosylation of PD-L1 and improved IHC
Many studies have demonstrated that the PD-L1 protein undergoes extensive N-glycosylation. Glycosylation, a PTM of membrane-bound proteins, regulates protein biosynthesis, folding, and stability by affecting protein structure and interactions with other molecules. It also plays a role in processes such as signal transduction, immunosuppression, and angiogenesis. However, the spatial hindrance of the large molecular structure of N-glycans may affect the recognition of PD-L1 by antibodies, leading to errors in the immunohistochemical detection of PD-L1 [15]. A study conducted by Heng Huan Lee et al. demonstrated that enzymatic removal of the glycan moiety on cell surface antigens significantly improved the affinity and signal intensity of anti-PD-L1 antibody binding. This deglycosylation process resulted in more accurate quantification of PD-L1 and improved clinical prognostic predictions [16]. Notably, this proposed sample deglycosylation method can be used to directly incorporate proteins into conventional immunohistochemical sample preparation via enzymatic reactions to eliminate protein n-junction glycosylation prior to antibody detection. However, the validation of this method needs to be accompanied by prospective data and standard operating procedures. Improving traditional IHC technology may be a new direction for improving the predictive efficacy of immunotherapy.
To overcome the masking effect of posttranslational modifications on PD-L1, fluorescence probes and targeted drug probes have also been extensively researched and applied for protein-specific detection [17, 18]. Compared to other targeted detection methods, such as gene sequencing and radioactive tracers, fluorescence probes offer unique advantages, including high selectivity, sensitivity, spatial and temporal resolution, low cost, and ease of operation.
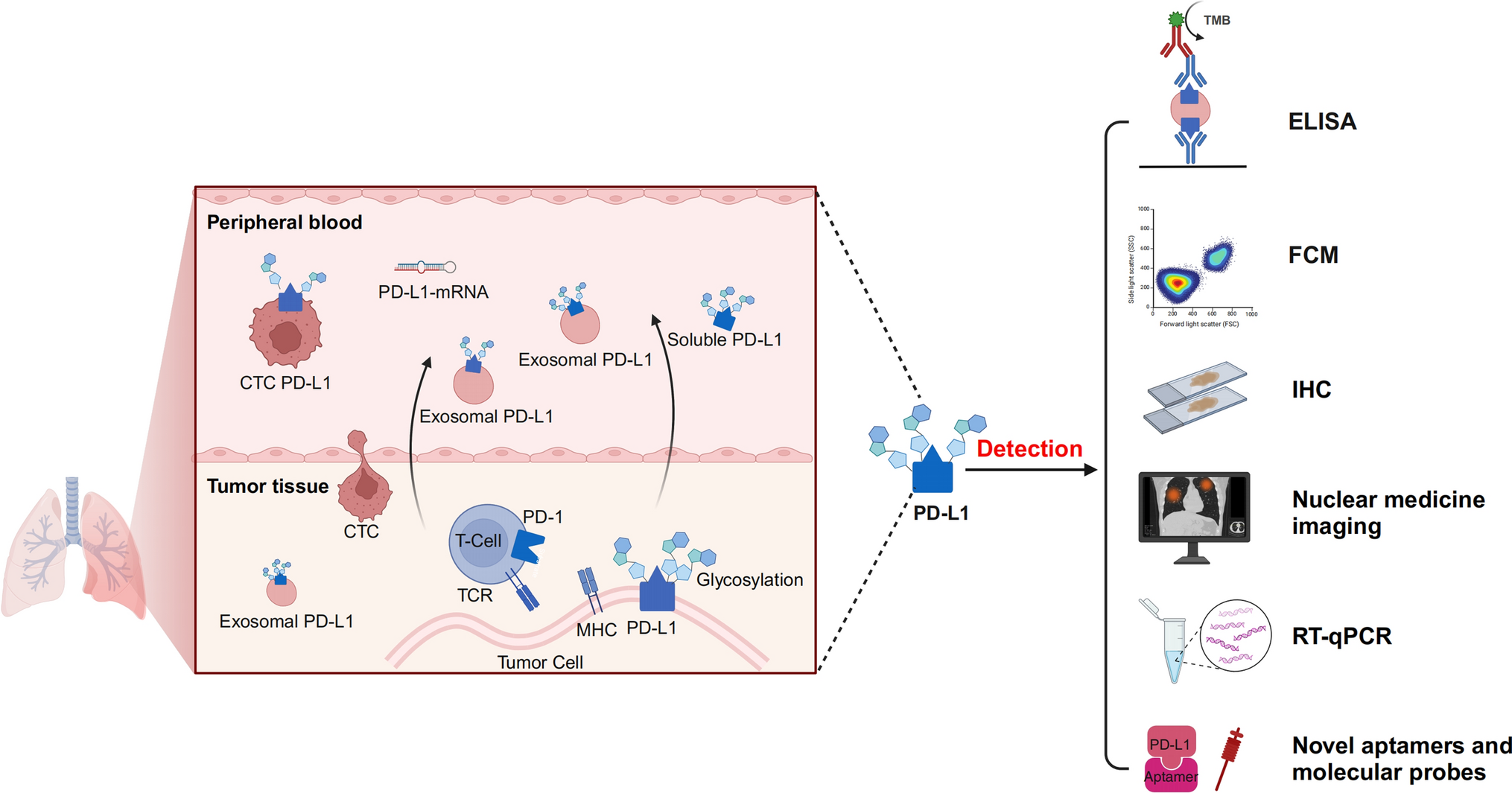
Detection of PD-L1 in peripheral blood
The utilization of circulating biomarkers in “liquid biopsy” has progressively garnered researchers' attention due to their non-invasive nature, dynamic monitoring capabilities, and ability to reflect the overall characteristics of the TME.
Soluble PD-L1 (sPD-L1) is the soluble form of the PD-L1 protein produced by tumor cells or other immune cells. It binds primarily to extracellular vesicles (exosomal PD-L1) or is expressed on the surface of circulating tumor cells (CTCs PD-L1). It can also exist in different forms, such as in its free form or bound to other proteins. Unlike PD-L1, which is expressed on the cell membrane, soluble PD-L1 does not require cell surface expression and can freely circulate in body fluids. sPD-L1 retains the programmed death protein 1 (PD-1)-binding domain and can competitively bind to PD-1 receptors, inhibiting the activation and function of T cells. It can, to some extent, represent the body's response to immune therapy. A study conducted by Zhou J et al. confirmed that the serum level of sPD-L1 in stage IV melanoma patients was elevated compared to that in healthy individuals and was associated with an increased likelihood of disease progression [19].
Notably, although many studies have indicated the clinical relevance of PD-L1 positive CTCs in various cancers, including NSCLC [14, 20,21,22,23], there is still controversy, and the analysis of CTCs is dependent on the use of different clones of anti-PD-L1 antibodies and CTCs enrichment techniques. Janning M et al. examined CTCs PD-L1 expression in 127 samples. They found that PD-L1 + CTCs increased in all patients as the disease progressed. However, the percentage of PD-L1 + CTCs was not related to the percentage of PD-L1 + tumor cells observed through IHC in the primary tumor tissue [24]. Furthermore, Kulasinghe and colleagues conducted a study utilizing blood samples from both head and neck cancer (HNC) patients and NSCLC patients for measurement of CTCs enrichment and IF staining of cell surface antigens. PD-L1-positive CTCs were found in 11 HNC patients (54.4%) and 11 NSCLC patients (64.7%). PD-L1 + CTCs were significantly associated with poor prognosis in HNC patients but not in advanced NSCLC patients [20].
Exosomes are small vesicles released by cells that contain various components, such as membrane lipids, proteins, and nucleic acids. They can be transferred to other cells through body fluids and facilitate intercellular communication. Research on the use of exosomes as novel diagnostic and prognostic biomarkers is pertinent for multiple diseases, including pancreatic cancer, ovarian cancer, breast cancer, and lung cancer [25,26,27]. Exosomal PD-L1 can mediate the therapeutic response of tumors to anti-PD-1/PD-L1 antibodies. It serves as a biomarker for monitoring disease progression and immune activity in NSCLC patients (Table 1). Compared to those in circulating tumor DNA (ctDNA) and CTCs, exosomes in peripheral blood have higher concentrations, good biological stability and compatibility, low immunogenicity, and low toxicity. Although there is no consensus on standardized exosome detection methods, various emerging detection methods have shown promising results [28, 29].
Table 1 Exosomal PD-L1 expression predicts the response to immunotherapy in NSCLC patientsELISA
ELISA is a classic method for detecting proteins in body fluids. This method can be divided into indirect detection, double-antibody sandwich detection and competitive binding detection methods. ELISA has a simple and standardized operation process, good stability and reproducibility, and is the first choice for sPD-L1 detection [30, 34].
In recent years, with in-depth research on sPD-L1 and its innovation in antibody synthesis, great progress has been made in the use of the double-antibody sandwich ELISA method. A Japanese study developed a new ELISA test system that has higher detection sensitivity in NSCLC patients than conventional ELISA. The PD-1-Ig fusion protein replaced the immobilized capture antibody in conventional ELISA and was able to quantitatively detect functional sPD-L1 with the ability to bind to PD-1 at 75 °C [35]. To improve antibody immobilization, Sareh Zhand et al. introduced a protective coating that made the detection limit and sensitivity 225 times and 15.12 times greater than those of commercial ELISA kits, respectively [36].
Flow cytometry
Flow cytometry (FCM), which is used to detect single cells, can also be used to detect exosomes. Whiteside's team used antibody-carrying droplets to bind to PD-L1-containing exosomes and analyzed the number of PD-L1-positive exosomes by FCM. They confirmed that tumor progression is related to the expression level of exosomal PD-L1, which is similar to what has been observed via IF [27]. In a study on pancreatic cancer, Alexander lux et al. used immunocytochemistry and FCM to explore the feasibility of circulating exosomal c-Met and PD-L1 as markers for the diagnosis and poor prognosis of pancreatic cancer [37]. To date, several flow cytometry methods, such as the Apogee A50 microflow cytometer, which is more suitable for detecting exosome proteins than traditional analyzers, have been designed for exosome detection on the market [38].
Exploration of new detection methods
In addition to traditional detection methods, the development of new technologies has increased the prospects for the clinical application of sPD-L1. The predictive utility of PD‐L1 + CTCs in a chemotherapy setting has been investigated by Kallergi and colleagues. The authors used an isolation by size of tumor cells (ISET) technique developed by Rarecells Diagnostics SAS to isolate CTCs. Subsequently, Giemsa staining and immunostaining were used to detect PD-1 + /PD-L1 + CTCs in metastatic NSCLC patients before and after chemotherapy. The results revealed that PD-1 + CTCs, rather than PD-L1 + CTCs, had potential clinical significance [39].
In recent years, with in-depth research on exosomes and innovations in the synthesis of sPD-L1 antibodies, great progress has been made in identifying exosomal PD-L1. Compared with traditional IHC, innovative photochemical and electrochemical immunoassay detection methods provide PD-L1 adaptors with better performance; these adaptors often have unique three-dimensional structures, are easy to modify, and have good stability and sensitivity [40, 41]. Huang et al. developed a uniform, small-volume, efficient, and sensitive exosomal PD-L1 quantification method. This method combines a newly evolved aptamer that can effectively bind PD-L1 and is less hindered by glycosylation. Therefore, it has higher sensitivity, faster reaction time and easier operation than the commonly used ELISA method [42]. Wei J et al. attached gold nanospheres (GNSs) to the bottom of an eight-well chamber slide to form a detection substrate. Then, the Cy5-labeled CD63 aptamer (i.e., capture probe) was modified on the GNSs through Au–S bonds. After the exosome-containing sample was added, the FAM-labeled PD-L1 aptamer (i.e., immunoprobe) was added to identify PD-L1 on the exosomes. Through three-color fluorescence colocalization of Cy5, DiI and FAM, high-sensitivity and high-reliability detection of PD-L1-overexpressing exosomes was achieved [43].
Surface-enhanced Raman scattering (SERS) is a commonly used Raman spectroscopic analysis method for the determination of samples adsorbed on the surface of colloidal metal particles. It has been applied in the biomedical field. Pang Y et al. proposed a method to capture and analyze exosomal PD-L1 directly from serum. Fe3O4@TiO2 nanoparticles are used to enrich exosomes, and then, based on personalized SERS signal analysis, exosomal PD-L1 is quantified, and the relationship between exosomal PD-L1 expression and immunotherapy response can be determined [44]. In addition, automatic centrifugal microfluidic disk systems and nanoplasma sandwich immunoassays, have also begun to be used for the detection of exosomal proteins, greatly improving accuracy [45, 46].
However, liquid biopsy has many limitations. The origin of sPD-L1 has not yet been determined. In contrast to tissue PD-L1 analysis, most liquid biopsy analyses for sPD-L1 use different detection antibodies with variable identification capabilities [19, 47]. The value of sPD-L1 analysis in clinical practice largely depends on the sensitivity and error rates of the separation and detection techniques used [23]. However, sPD-L1 testing is indeed a clinical alternative, especially for patients for whom adequate tumor specimens cannot be obtained.
Genetic detection of PD-L1
Plasma PD-L1 mRNA contains many genetic materials similar to those derived from tumor cells. Some of these substances are involved in cell cycle regulation, and some are related to important cellular activities, such as chromosome segregation, proliferation and migration. The prognostic prediction effect of extracellular vesicle (EV)-mRNA biomarkers may be better than that of EV-based protein biomarkers. Simonsen et al. evaluated PD-L1 expression in tumor samples from 42 NSCLC patients by IHC and detection of the PD-L1 encoding gene CD274. The results showed that gene-based assessment of PD-L1 expression was also consistent with the initial IHC assessment [48]. Another study used quantitative reverse transcription polymerase chain reaction (RT-qPCR) to detect the relationship between four target immune genes, CD274, programmed cell death 1 ligand 2 (PDCD1LG2), CD8A and interferon regulatory factor 1 (IRF1), and ICIs treatment response in 122 patients with advanced NSCLC. Researchers have shown that high mRNA encoding immune checkpoint protein expression levels are associated with improved long-term survival and OS. Most importantly, low PD-L1 mRNA levels have a strong negative predictive value for the absence of long-term benefits [49]. One study proposed an immunogold biochip as a noninvasive alternative to quantify the expression of PD-L1 protein and mRNA on vesicles. The method is 1,000 times more sensitive than conventional ELISA and RT-qPCR [50].
PD-L1 mRNA, a gene-level biomarker, has great potential for guiding immunotherapy and predicting efficacy [51]. There are still differences between the transcription of the mRNA and the actual translation of the protein, which can lead to errors in test results. Whether this approach can compensate for limitations such as insufficient clinical specimen collection requires further experimental research and data analysis.
Imaging detection of PD-L1
Standard methods for detecting PD-L1 on tissues, such as immunohistochemistry and ELISA, are often insufficient to accurately and comprehensively evaluate the expression of PD-L1, and the measurement of circulating markers lacks representativeness. Research on radiomics provides new ideas to solve this problem, achieving accurate, comprehensive and dynamic detection of PD-L1 expression levels in tumors through noninvasive methods. To date, nuclear medicine imaging relies mainly on positron emission tomography (PET) and single-photon emission computed tomography (SPECT). In terms of nuclear imaging detection of PD-L1, the development of new tracers is the key to this research. These tracers usually consist of two parts: radionuclides and PD-L1 ligands (monoclonal antibodies, monopolar antibodies, connexins, phages, peptides and small molecules).
Radiolabeled anti-PD-L1 antibodies
Radiolabeled anti-PD-L1 antibodies are currently the most commonly used type of nuclear medicine imaging probe. Anti-PD-L1 antibodies, such as thallium-99 m (99mTc) or technetium-99 (99Tc), are labeled with radioactive isotopes to observe their distribution in the body through PET or SPECT. Due to their high specificity, high affinity and availability, monoclonal antibodies have been shown to be highly reliable PD-L1 ligands. In 2015, Natarajan et al. developed a tracer based on the anti-mouse PD-1 monoclonal antibody 64Cu-DOTA-PD-1 and used PET imaging tracers to detect the expression of PD-1 in vivo for the first time [52]. Bensch et al. conducted the first human study to evaluate the feasibility of PET with zirconium-89-labeled atezolizumab in 2018. Preliminary results suggest that the assessment of PD-L1 status via molecularPET may better predict patient clinical response than can the use of predictive biomarkers from immunohistochemistry or RNA-seq [53].
Radiolabeled small molecule ligands for PD-L1
Compared with the shortcomings of antibodies, such as large molecular weight, long half-life, and slow generation of high-contrast images, some current nonmonoclonal antibody PD-L1 small molecule ligands, including connexins, appendages, peptides, small proteins, and antibody fragments, may act as tracers with lower molecular weights, higher tumor uptake rates, and rapid clearance.
Broos et al. developed the small molecular weight (15 kDa) single-domain antibody sdAb K2, which has high specificity for PD-L1. SPECT/CT images with a high signal-to-noise ratio could be generated within 1 h in mice. Notably, the sdAb K2 also has the ability to antagonize the interaction between PD-1 and PD-L1, which has potential therapeutic value [54]. In addition, the recently emerged immuno-SPECT probe [99mTc] Tc-HYNIC-KN035 also performed well in assessing the expression of PD-L1. The probe used was the nanobody KN035, which has high specificity and affinity for PD-L1, coupled to the chelator succinyl 6-hydrazinonicotinate and subsequently labeled with the radionuclide 99mTc [55]. Compared with other reported tracers, [99mTc] Tc-HYNIC-KN035 exhibited sustained high tumor uptake and a satisfactory target-to-background ratio [56]. Donnelly et al. used the Adnectin molecule (BMS-986192), which can detect the expression of PD-L1 in animal tumor models, to develop a tracer with high binding affinity for PD-L1, 18F-BMS-986192 [57]. Subsequent small-molecule tracers, such as 68 Ga-BMS-986192 and 68 Ga-NODA-BMS986192, have been optimized by 18F-BMS-986192, which has stronger automation and better stability [58, 59]. In addition, small molecule compounds such as radioactively labeled PD-L1-binding peptides and phages can also bind to PD-L1 and be enriched in tumor tissues, thereby facilitating PD-L1 imaging [60,61,62,63].
Radionuclides, such as 68 Ga, 18F, 99mTc, 64Cu, 89Zr, 124I, and 125I, have been used to label ligands for the production of various tracers. 18F is commonly used for PET, while 99mTc is more commonly used for SPECT. The characteristics of radioactive elements themselves also cause problems such as a half-life that is too long or too short, delayed clearance, long imaging time, and excessive radiation dose to healthy organs [64]. Therefore, choosing the appropriate radionuclide is crucial when manufacturing tracers.
Artificial intelligence (AI) model detection of PD-L1
With the development of AI technology, the “Internet + ” model is being increasingly applied in clinical medical research. In 2023, two academic centers conducted a retrospective, multicenter study on 385 patients with advanced NSCLC who were suitable for treatment with ICIs. They evaluated combinations of machine learning algorithms with different feature selection methods and constructed imaging-based PD-L1 and PFS prediction models using radiological features extracted from preprocessed CT scans. Researchers found that logistic regression with ReliefF feature selection and support vector machine (SVM) with analysis of variance (ANOVA) with test feature selection were the best models for predicting PD-L1 expression and PFS [65]. Additionally, Shani Ben Dori et al. used machine learning models to explore the risk of inaccurate diagnosis of PD-L1 expression. The results show that the proposed model can be used to identify the risk of PD-L1 prediction errors, with the error rate increasing significantly when the PD-L1 expression ratio approaches the threshold [66].
AI technology has opened a new field for the development of noninvasive biomarkers. Previous studies have also shown that it is feasible to use AI deep learning to evaluate PD-L1 expression in NSCLC and predict the response to ICIs. Patients with shorter survival times are quickly and noninvasively identified by AI models, allowing clinicians to effectively select alternative optimal treatment strategies [67].

留言 (0)