
記住我
This single-center retrospective cohort study was conducted at the University Medical Center Utrecht (UMCU) between 01-03-2021 and 01-11-2022. All patients included in the study were subjected to neutrophil phenotyping as a standard-of-care procedure following presentation at the trauma bay. Outcomes of flow cytometry were prospectively collected, whereas patient data were retrospectively collected from electronic patient files as well as the Dutch trauma registry. This study was approved by the UMCU ethical review committee (21-1016_AQUIretro2). The processing and storage of data were in accordance with privacy and ethics regulations. The STROBE statement was adhered in order to assure accurate documentation of methods, results, and discussion (appendix 1).
Patient selectionAll trauma patients ≥ 18 years of age admitted to the trauma unit from whom a diagnostic blood sample for determination of neutrophil phenotypes was taken were included. From this existing retrospective, observational cohort database, patients with TBI were identified using data from the trauma registry. There were no exclusion criteria regarding systemic inflammatory responses or metabolic syndromes, as immunosuppressed patients do not show significant differences in numbers of neutrophils subsets as previously described by de Fraiture et al. [4] Lastly, comorbidities, alcohol and drugs abuse were not determined as they are likely missed due to the retrospective design of this study, makingthese unreliable exclusion criteria.
Patients were categorized in four groups: isolated trauma with TBI, isolated trauma without TBI, multitrauma with TBI and multitrauma without TBI. Patients who did not survive or were transferred to another hospital were excluded from the analysis on infectious complications unless they already had developed an infection prior to their transfer or death.
Patient population definitionIsolated TBI patients suffered from an isolated head trauma with Abbreviated Injury Scale (AIS) head or skull ≥ 2 and no other AIS > 1. Patients were also included if they had additional facial fractures with AIS > 1 but excluded if they only suffered facial fractures without TBI.
Isolated non-TBI patients suffered from an isolated injury of AIS ≥ 2 in only one body region, which was not TBI and no other AIS > 1.
Multitrauma TBI patients suffered from both TBI AIS ≥ 2 and ≥ 1 other injury to any other region of AIS ≥ 2, with an ISS ≥ 16 [11].
Multitrauma non-TBI patients suffered from injuries of AIS ≥ 2 in ≥ 2 body regions, which was not the head or skull, with an ISS ≥ 16 [11].
Data collectionPatient characteristics and outcomes were collected using the trauma registry and supplemented by the patient’s medical file. The following data was collected: age, gender, pre-existing comorbidities, date of trauma, trauma mechanism, type of injury, AIS, ISS, Glasgow Coma Score (GCS) directly after trauma, Intensive Care Unit (ICU) days, Medium Care (MC) days, Length Of hospital Stay (LOS), ventilation days, timing of surgical procedures, in-hospital mortality, and infectious complications. Data on neutrophil surface receptor markers CD16 and CD62L directly after trauma was also collected. Infectious complications were reported in patient’s medical files when they were diagnosed by a clinical practitioner based on clinical signs and laboratory findings (e.g. CRP and leukocyte counts). Imaging or microbiological finds were included in the diagnosis if applicable. Infectious complications were included in this study when the diagnosis was reported in the patient’s medical file in combination with administration of appropriate treatment according to hospital guidelines. Only infections occurring > 48 h after admission and before hospital discharge were included. Moreover, all patients with an expected ICU stay > 48 h received Selective Digestive Decontamination (SDD) in the form of SDD paste consisting of polymyxin B, nystatin and tobramycin. Additionally, intravenous ceftriaxone was administered for 4 days.
Method of calculating injury severity scoreISS is calculated using AIS. Each individual injury is assigned a body region and a severity scale from 1 to 5. Scale 1 is equivalent to minor injury, 2 to moderate injury, 3 to serious injury, 4 to severe injury, 5 to critical injury and 6 to maximal injury [11,12,13]. Scoring is dependent on type of injury as well as extensiveness. For example, an extensive traumatic subarachnoid hemorrhage with coma can be scored an AIS 5, yet a minor traumatic subarachnoid hemorrhage without coma can be scored an AIS 2.
Sample acquisition and AQUIOS CL® flow cytometryBlood samples were obtained directly after patient arrival at the trauma bay. One 4mL sodium-heparin tube (Greiner Bio-One GmbH, Kremsmünster, Austria) of blood was collected for granulocyte phenotyping. Subsequently, the blood tube was inserted in the AQUIOS CL® “load & go” flow cytometer (Beckman Coulter Life Sciences, Miami, FL, USA) positioned near the shock room. The AQUIOS CL® “load & go” flow cytometer examines the fluorescence of antibody/fluorochrome-combinations specific for different target proteins on the surface of immune cells in the blood, following the protocol described in de Fraiture et al. [4].
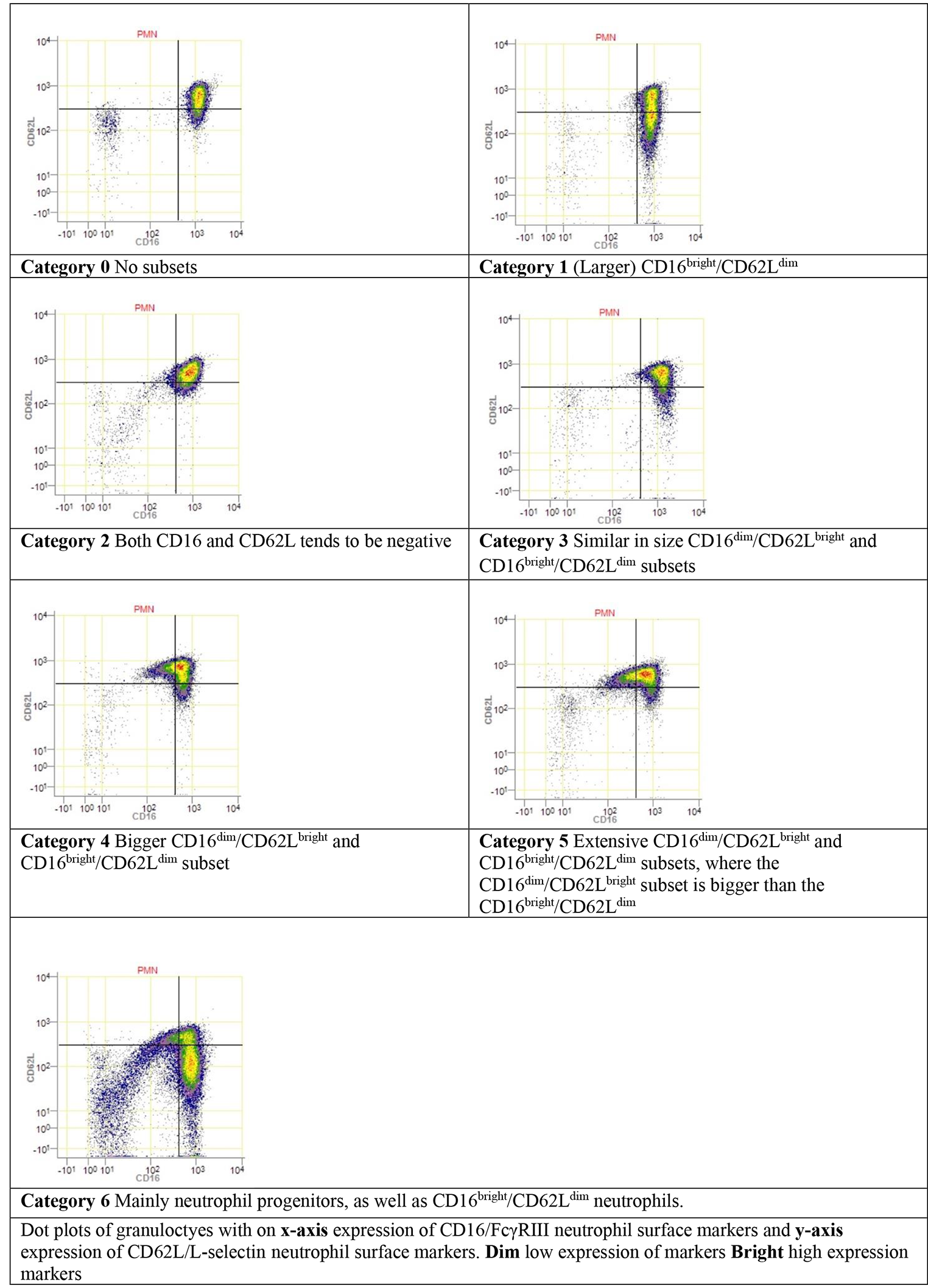
Neutrophil subset categorizationDuring acute injury induced inflammation, neutrophils can be divided into different phenotype subsets, based on the expression of specific surface proteins (CD16/FcγRIII and CD62L/L-selectin) [4, 14]. Upon acute inflammation two additional phenotypes are found in the peripheral blood. CD16dim/CD62Lbright neutrophil subsets represent the immature banded phenotype, which are most potent in containing pathogens. CD16bright/CD62Ldim represent the hypersegmented neutrophil phenotype, which show impaired intracellular bacteria killing and possibly have a more immune regulatory function [14].
For each patient, a 2-dimensional CD16/CD62L dot plot was assigned a category 0 to 6 by visual assessment based on the presence of CD16dim/CD62Lbright and CD16bright/CD62Ldim neutrophil subsets, as previously described by de Fraiture et al. [4] Fig. 1 shows the different categories. Category 0 shows no subsets, category 1 only shows a CD16bright/CD62Ldim subset and category 2 shows a subset in the lower left quadrant of the plot which tends to be both CD16 and CD62L negative. Categories 3, 4 and 5 show increasing presence of both CD16dim/CD62Lbright and CD16bright/CD62Ldim neutrophil subsets. In category 5, the presence of CD16dim/CD62Lbright are more distinct than CD16bright/CD62Ldim neutrophil subsets. Category 6 shows the presence of the CD16bright/CD62Ldim subset as well as neutrophil progenitors (CD16dim/CD62Ldim). In categories ≥ 3, the categorical number increases with severity of trauma and the concurrent extent of the immune response [4]. The categorization was done by visual assessment by 2 authors. If consensus could not be reached, a third author was consulted.
Fig. 1
Illustration of expression of neutrophil receptor markers CD16 and CD62L for each category
Statistical analysisStatistical analysis was done using R software for statistical computing (version 3.3.2.) [15].
Baseline characteristics and outcomes were compared using Mann-Whitney-Wilcoxon test for numerical variables and Chi-square test for categorical variables. Number of TBI and non-TBI patients, their median ISS, and the development of infections in each neutrophil category were compared using Mann-Whitney-Wilcoxon and Chi-square test.
留言 (0)