Use of MRI to determine age
Many studies have repeatedly demonstrated that ossification of the epiphysis is a process from which information can be used to estimate age [17]. For instance, Fan et al. showed that chronological age correlates well with ossification of the epiphyses in the knee region [18]. However, many earlier studies relied on X-ray images analyzed according to the standards of Greulich and Pyle or Tanner and Whitehouse [1, 19, 20].
X-ray images of the hand, orthopantomography of the jaw and CT examinations of the clavicle epiphyses are included in the AGFAD recommendations. These examinations for forensic age assessment are not medically indicated. The use of ionizing radiation for forensic age determination is always the subject of controversy. Even if the radiation exposure is low, especially for hand X-rays, it is desirable to avoid exposure. Alternatively, radiation-free imaging procedures analogous to the recommendations of the AGFAD, such as sonography of the wrist and MRI of the clavicle, are available [19, 21, 22]. The use of MRI of other body regions, such as the knee joint for forensic age diagnosis, is also the subject of numerous studies [23].
However, in addition to the advantage that ionizing radiation can be avoided, other factors must also be considered. These include longer scanning times, relative contraindications, higher costs and lower availability. In addition, patient age, compliance and any phobic reactions, which can lead to artifacts and limited assessability, must also be taken into account [24].
Methods focusing on the evaluation of MRI images of the knee are based on the evaluation standards of Kellinghaus and Schmeling [6, 25]. The ossification process of the knee and the good correlation with chronological age could be demonstrated by analyzing MRI images as well as X-ray images. In addition, MRI, being a cross-sectional imaging technique, provides multiple two-dimensional images of body areas, offering more comprehensive information compared to conventional X-ray projection images. This makes it possible to recognize incomplete or early-stage epiphyseal fusion on at least one image within the series. Conventional X-ray images offer only a singular perspective for analysis (24; 25). Therefore, age estimation using MRI scans should be considered as an alternative to X-ray images. As Fan et al. correctly stated, the knee joint offers the possibility to examine three epiphyses of long bones (distal femur, proximal tibia and proximal fibula) in one image [18]. All three long bones were assessed in the current study. While Ottow et al. expressed concerns about the reliability of assessing the proximal fibula epiphysis due to a limited series of images where it appears [5], our results demonstrate that the ossification of the fibular epiphysis can indeed be reliably evaluated. However, the results of the proximal fibular epiphysis are different to the results of the proximal tibial and distal femoral epiphysis.
Duration of the examination and evaluation
It takes a few minutes to produce an MRI image. In our study the pure acquisition time for the T1 TSE was 2 min 54 s (3 Tesla), 3 min 1 s (1,5 Tesla) and the T2 TIRM 2 min 26 s, respectively. According to the literature, a pure acquisition time of 2 min and 45 s applies for the T1-VIBE sequence (Volumetric Interpolated Breathhold Examination) for age estimation of the hand. In addition, there is an undefined period of time for the correct preparation of the patient [10]. In this context, it should also be mentioned that image acquisition in general has become faster, partly due to the use of artificial intelligence [26]. For instance, a study by Neumayer et al. demonstrated a significant reduction in acquisition time for MRI-based forensic age estimation of the hand through data undersampling [27]. It is important to note that the knee joint is an easily accessible region, which is less susceptible to movement artefacts and often offers no variations, unlike the medial epiphyses of the clavicles [24]. The evaluation according to Ottow et al. required an average time of 8.8 s. The evaluation according to Vieth et al. required an average time span of 10.6 s, this longer time span is due to the observation of T1 and additionally T2 sequences at stage 5 and stage 6.
Results from Vieth et al.
The results of this study indicate that the proposed method by Vieth et al. is effective in accurately determining age limits. Specifically, age limits 14 and 21 were successfully established for both sexes. The age limit 18 could be determined for the female patients with stages 2–4. If stage 6 was classified at the distal femur in both sexes, all patients were older than 18 and also older than 21 years, even if the minimum age of stage 6 was very close to the age limit of 21 (female 21.05 and male 21.04).
The statistical bias described by Vieth et al. at the age limits of 14 and 21 years was not observed in this study, as the upper age limit for this study was 28 years instead of 24 years, as in Vieth et al. Furthermore, the present study has a sufficient number (N = 77) of cases in stage 6. In addition, the lower cut-off for the entire cohort in this study was also set at 10 years instead of the lower cut-off of 12 years selected by Vieth et al. Thereby, the selection bias for stages 2 and 3 is reduced. The proposal of Vieth et al. to consider the minimum age for stages 2 and 3 as well as the maximum age for stage 6 as artificial limits could be confirmed, as the limits adjusted with the extension of the age limits.
The results of Vieth et al., which were presented using the “minimum age concept”, were confirmed in the present study. For the distal femur, it was found that stage 6 was assigned in all cases to persons over 18 years of age in both sexes, as the youngest age was 21.05 years for females and 21.04 years for males. Stage 4 could always be assigned to males over 14 years of age, as the youngest age was 15.67 years. Stage 5 could always be assigned to females over 14 years of age, as the youngest age was 15.15 years. When considering the proximal tibia and fibula, stage 5 was assigned to females over 14 years of age in all cases and stage 4 was assigned to males over 14 years of age in all cases. Stage 6 could only be assigned for the proximal tibia in all cases to persons over 18 years of age for both sexes.
To summarise, 100% of stage 2 patients were under 14 years of age in both sexes and 100% of stage 3 patients were under 21 years of age in both sexes. Stage 4 could always be assigned to males over 14 years of age and stage 5 could always be assigned to females over 14 years of age. With stage 6, the completion of the age of 21 could be determined 100% of the time in both sexes. These results apply when the distal femur is assessed. When considering the proximal tibia and fibula, stage 5 was assigned to females over 14 years of age in all cases and stage 4 was assigned to males over 14 years of age in all cases. In both sexes, all individuals in stage 6 were older than 18 years only at the proximal tibia. For males, the minimum age of 18.34 years in stage 6 was also very close to the age limit of 18 years. This once again illustrates the importance of exceeding or falling below certain stages with regard to forensic age determination. Furthermore, it was observed that for each stage of the three long bones reached, the mean age was younger in females than in males. This finding has also been documented in other studies [3, 5, 18, 28,29,30,31].
It is important to note that if a stage cannot be assigned, the chronological age of the person does not automatically fall beyond the corresponding age limit. For example, a person with stage 2 is 100% under 14 years old, but it should not be assumed that if stage 2 is not assigned, the person is over 14 years old.
Results from Ottow et al.
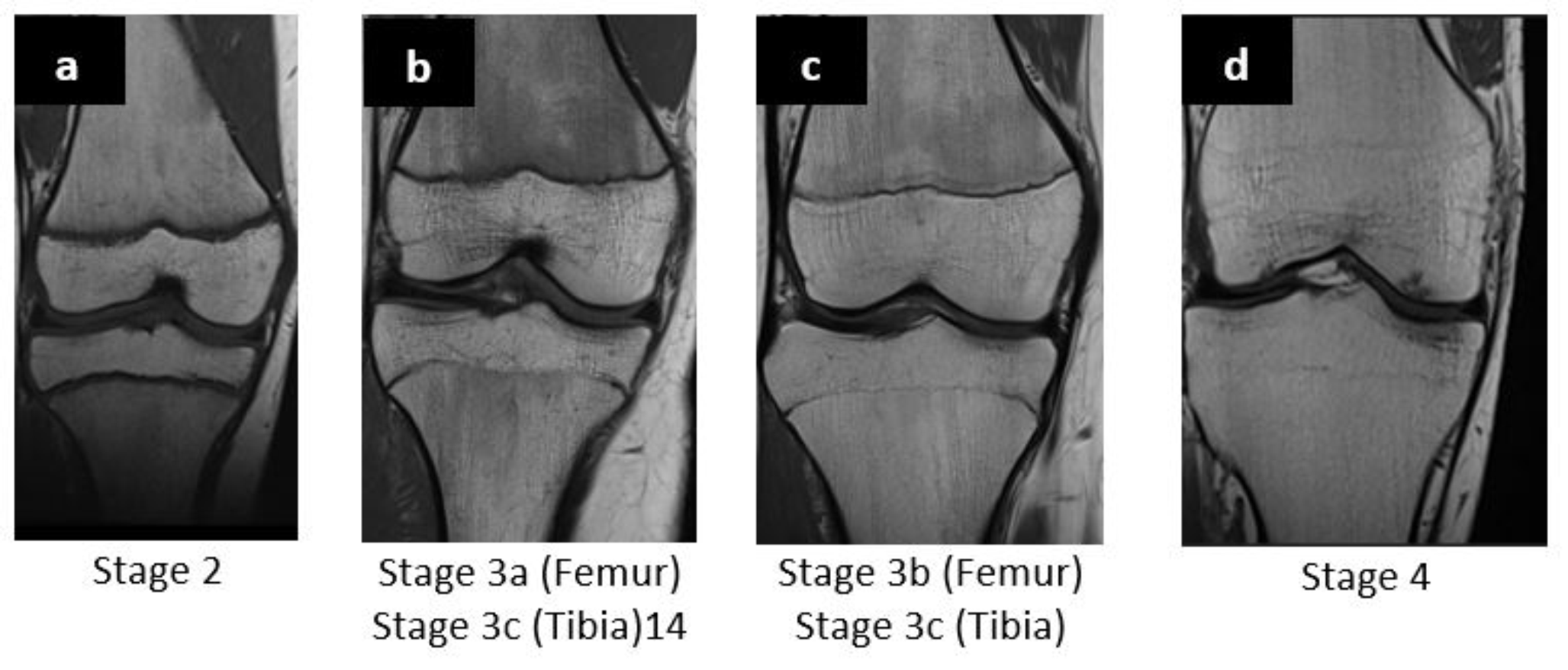
Ottow et al. found that significant differences between women and men in the ossification process of the distal femur are only found from the age of 13. Female patients reached stage 3b at 14.73 years, while male patients only reached stage 3a at 17.77 years [31, 32]. Similar results can be reported in the present study. According to Ottow et al., female patients reached stage 2c at 12.11 years, in the present study at 10.57 years (mean average age of the patients was 10.64 years). Stage 3a was reached at 13.39 years (Ottow et al.) and in the present study at 10.18 years (mean average age 12.91 years). The variations in minimum age across the different stages can be explained by the diverse age groups considered, leading to potential biases in the results, especially close to the age limits. From stage 3b onwards, the results of Ottow et al. were confirmed in that a significant difference between the sexes could be recognized after the age of 13.
According to Ottow et al., the age of 14 years in males can be determined via stage 3c of the distal femoral epiphysis and the proximal tibial epiphysis. Similar results were obtained by Krämer et al. and partly by Jopp et al. [5, 30, 33]. Krämer et al. showed that the completion of the 14th year of life could be determined with stage 4 in females and with stage 3c in males [30]. The results of the present study are consistent with the data from the studies described above, as the age of 14 years could be determined for the distal femur in males with stage 3c. The youngest age in this case was 14.18 years. The same applies to the proximal tibia and fibula, in both cases, the youngest age of males with stage 3c was 14.18 years. However, in contrast to the results of other studies, in the present study the completion of the 14th year of life could also be determined for the distal femur in females with stage 3c, as the youngest age was 14.25 years. Based on the assessment of the proximal tibia and fibula, it is possible to identify females over 14 years with stage 4. Persons under 14 years could be identified by stage 2c in all three long bones. The exact age limits of all stages and long bones are shown in Fig. 6.
Ottow et al. also described that it was not possible to reliably determine the age of 18 years in both sexes due to the defined stages and the associated sub-stages, as the earliest documented stage 4 of the distal femoral epiphysis in males was under 18 years in several cases. The results of the present study contradict the finding described above. Among 356 cases who were under 18 years of age at the time of the study, 222 cases were categorized as stage 2c, 3a or 3b. Subjects with stage 3c were always under 21 years old. Stage 4 was assigned to patients over 18 years of age in 89.2% of cases and stage 5 was assigned to patients over 21 years of age in 100% of cases. Ottow et al. assumed that the minimum age for stage 5 was over 24 years for both sexes. Due to their chosen age range of 12 years to 24 years, a bias in the results close to the age limits was assumed. These observations and assumptions are consistent with those of Krämer et al. [19, 30, 31]. In the present study, due to the extension of the maximum cut-off value to 28 years, it could be shown that stage 5 is above the age of 21 years in both sexes. Stage 1-2b could not be assigned despite the minimum threshold of 10 years.
In summary, upon closer examination, not all the results from Ottow et al. could be confirmed in our study. However, it was possible to determine that if only the distal femur was considered, 100% of under 14-year-olds could be identified for both sexes using stage 2c and 100% of under 18-year-olds for both sexes using stage 3a. Stage 3b could be assigned 100% to females under the age of 18. Stage 3c was assigned 100% to over 14-year-olds on the one hand and always to under 21-year-olds in both sexes on the other. Stage 5 could be assigned to males over the age of 21. Accordingly, the classification by Ottow et al. was able to determine the completion of the 18th and 21st year of life in both sexes based on the distal femur.
When looking at the proximal tibia and fibula, sex-specific differences were recognizable, while stage 3c could always be assigned to males over 14 years of age, stage 4 was assigned to females over 14 years of age. Stage 5 could be assigned to persons over 21 years of age in both sexes. Furthermore, it was observed in other studies that for each stage of the three tubular bones reached, the mean age was lower in females than in males. As described by Ottow et al., this corresponds to the results of several studies [3, 5, 18, 28,29,30]. It should also be noted at this point that if, for example, stage 3a is assigned, the person is 100% under 18 years of age, but it cannot be stated that at higher stages the person is automatically over 18 years of age. The definition of the age groups must therefore be considered when interpreting the different stages.
One would assume similar minimum ages in both classifications for the respective stages considering that stage 4 (Ottow et al.) and stage 5 (Vieth et al.) are basically the same in the T1w-sequence, when ignoring the water sensitive sequence. In males, the minimum age in stage 4 (Ottow et al.) was lower with 12.31 years for all three bones than in stage 5 (Vieth et al.) with 13.96 years. This difference could possibly be due to the additional assessment of the TIRM-sequence for the classification according to Vieth et al. In females, the minimum age was the same for all three bones and the maximum age differed only minimally by 0.09 years.
The two referenced classifications were initially applied to coronal MR images. In our study, both coronal and sagittal orientations were included in the analysis. This could be a possible reason for the deviations in the minimum ages, even though the classifications primarily refer to the assessment of the epiphysis and were further developed from the classification of the ossification of the epiphysis of the clavicle.
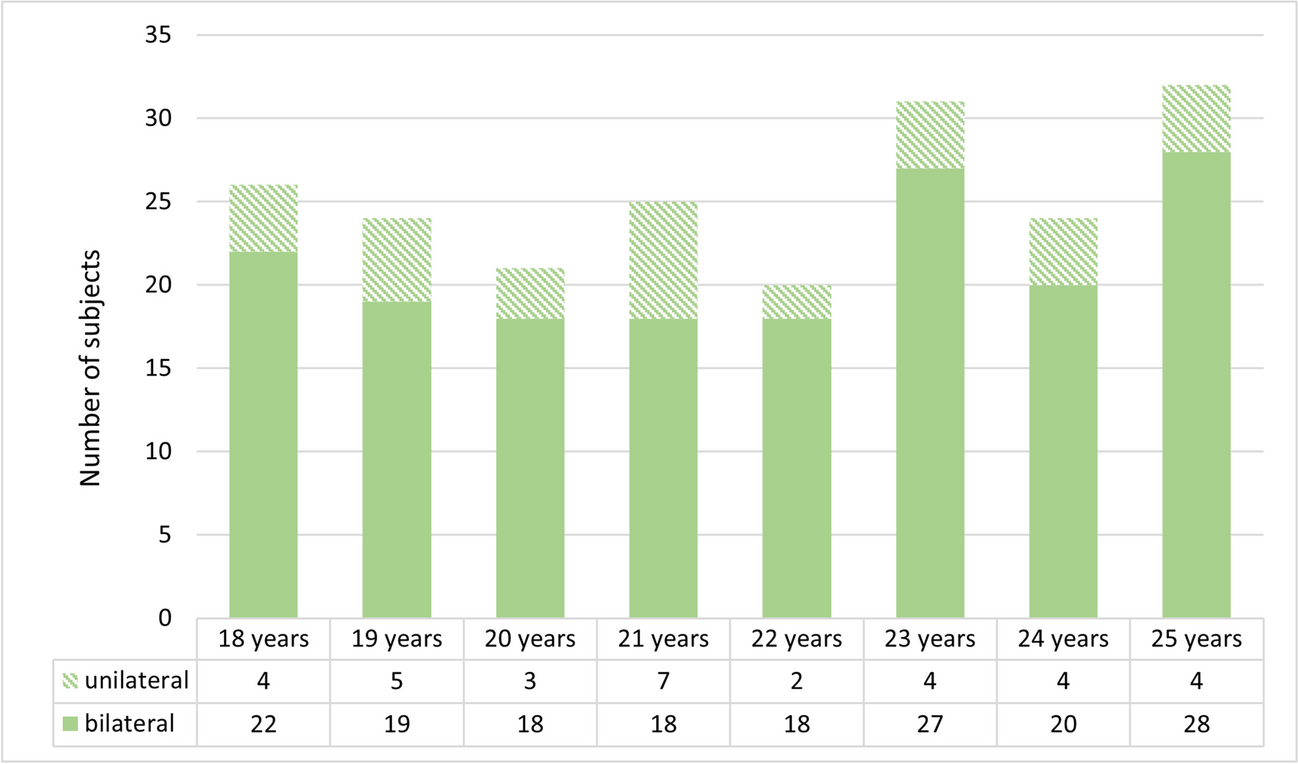
In the “classic” method of bone age estimation following the Greulich and Pyle (GP) standards using hand radiographs, the non-dominant left side is typically utilized. This approach estimates bone age by comparing the radiographs of the subject’s non-dominant wrist with the nearest matching reference radiographs provided in the atlas. The rationale behind this choice lies in the fact that the majority of individuals are right-dominant, making the left hand less susceptible to traumatic changes or deformities. While some studies have reported differences in bone age between the right and left hand in direct comparisons, others have found no such distinctions [34,35,36,37,38]. In our current study, even among the 62 patients who underwent MRI scans of both knee joints on the same day, the stage was consistently identical for both sides, as per the criteria outlined by Ottow et al. and Vieth et al.
The intra-observer variability results, although slightly lower compared to Ottow et al. and Vieth et al., still demonstrate a high level of accuracy, rating as very good. Notably, despite differences in experience between the two investigators, the intra-observer variability results remained consistently very good. These findings suggest that both classifications yield reliable results even with varying levels of experience. In a study concerning bone age determination utilizing the Greulich/Pyle method, Lynnerup et al. demonstrated that examiner experience did not significantly impact evaluation accuracy in a direct comparison [39]. However, whether this principle extends to MR classifications, as employed in our study, warrants further investigation through additional comparative studies.
In our study, we employed MR sequences as outlined in the original studies by Ottow et al. and Vieth et al., utilizing T1 turbo spin-echo (TSE) and T2 TSE with fat suppression via spectral pre-saturation with inversion recovery (SPIR). T2-weighted images proved crucial, particularly in distinguishing between stage 5 and stage 6 according to the Vieth classification. Meanwhile, T1-weighted images offered exceptional clarity in analyzing ossified parts of the epiphysis. The utilization of fat-suppressed MR images generally enhance sensitivity for detecting subchondral bone marrow lesions. Furthermore, for bone age estimation, these images facilitate the visualization of fluid signals at the epiphyseal scar, aiding in the differentiation of stages 5 and 6 as per Vieth et al. Beside insensitivity to magnetic field inhomogenity it is important to acknowledge extended imaging durationand lower signal-to-noise ratio compared to alternative fat suppression techniques [40].
Instead of utilizing the fat-suppressed T2-weighted images recommended by Vieth et al., Has et al. opted for proton-weighted sequences (PD) without direct comparison to the fat suppression technique via SPIR as proposed in the original publication [41]. While articular cartilage differs significantly, the vascularization of epiphyseal cartilage offers an opportunity for imaging during human skeletal development. In an ex vivo study, Ellermann et al. successfully visualized vascularized epiphyseal cartilage using gradient-recalled-echo sequences (GRE), allowing for a detailed differentiation between ossified and cartilaginous segments of the epiphysis [42]. This enhanced visualization of the cartilaginous parts could significantly improve differentiation of various stages, particularly in stages 3 a-c by Ottow et al.
A recent review on MRI analysis of the knee for bone age determination underscored the heterogeneity of study populations, grading systems, and MR protocols, leading to limited comparability [43]. Future studies should aim to directly compare the advantages and disadvantages of different MR sequences in age determination to establish recommended MR protocols. This comparative approach would offer valuable insights into optimizing imaging techniques for more accurate bone age assessment.
Limitations
The impact of actual illnesses or malnutrition in adolescents and young adults on epiphyseal growth requires careful evaluation. In the study at hand, all known potentially influencing factors were documented in the categorization, but not considered in detail. Table 1 lists all indications for the MRI scans. The present study is subject to certain limitations, notably the absence of recorded systemic diseases and medication histories of the included patients. Such factors could potentially impact the ossification process of the epiphysis. Among these variables are growth disorders, hormone therapy, steroid usage, and chemotherapy, all of which may exert significant influence on the epiphyseal ossification.
Despite not taking the individual diseases into account, a reliable categorization of the stages was possible. In the case of pathologies in the used MRIs that impaired the assessment of the epiphyseal joints, the examination was excluded.
The classifications utilized in this study were originally based on MRIs of healthy German volunteers and subsequently applied to a cohort of German patients. Notably, alternative classification systems, like that proposed by Dedouit et al., were not incorporated. Future investigations should delve into comparing these classification methodologies and extend the analysis to encompass diverse ethnic backgrounds [28, 43]. However, the present study shows that the application of classification systems developed on healthy persons can be applied well to German patients with different indications for MRI scans, as the results were largely confirmed.
Another crucial consideration is the assumed correlation between ethnicity and socioeconomic factors influencing bone growth [18, 28, 44]. However, there is scientific disagreement regarding which of the two factors influence bone growth. Since the actual patients in the studies have a high developmental status, the ossification process is completed earlier than patients with lower socioeconomic status. Consequently, an underestimation of age may not be disadvantageous from a forensic point of view [25, 44, 45]. Moreover, defining an individual’s socioeconomic status poses challenges, and even with a successful basic definition, clear assessment and proof can be challenging, especially in the case of refugees.






留言 (0)