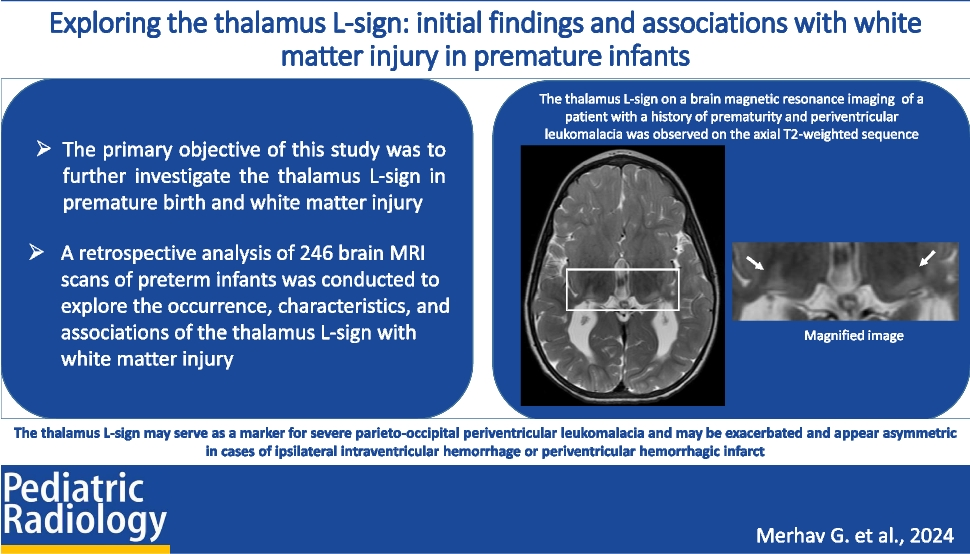
In this study, we investigated the incidence of the thalamus L-sign on brain MRI scans in a cohort of patients with a history of prematurity. Our analysis revealed that the L-sign, a radiological feature characterized by changes in the posterior and lateral margins of the thalamus, was notably associated with posterior parieto-occipital PVL. This association was particularly strong in cases of severe PVL, wherein the L-sign was detected with the greatest frequency. Notably, in our cohort, an asymmetric presentation of the L-sign was documented in four cases. Each of these cases had experienced a preceding ipsilateral IVH of grade III or a periventricular hemorrhagic infarction, accompanied by more pronounced white matter injury on the affected side.
Prematurity-related thalamic injury is a well-known phenomenon and may manifest through secondary mechanisms, involving anterograde or retrograde (trans-synaptic) damage, or via direct damage to the thalamic structures, as evidenced by neuropathological and radiological investigations revealing volumetric reduction and gliosis [9, 13,14,15]. The thalamus L-sign, along with its link to posterior parieto-occipital parenchymal damage, suggests that these injuries primarily occur as secondary effects rather than direct insults to the thalami. Advanced neuroimaging techniques, including functional MRI and diffusion tensor imaging, have clarified this relationship by highlighting the specialized connectivity between the posterior-lateral thalamic regions and the parieto-occipital cortex [16]. This connectivity is crucial for visual processing and spatial attention, and disruptions can result in impairments in visual perception, spatial awareness, and attentional control [11].
As previously described by Misser et al. [1], the thalamus L-sign may be indicative of parieto-occipital cortical injury, which is observable in situations of partial prolonged HII and further exacerbated by additional hypoglycemia-induced parenchymal damage. In the context of prematurity, thalamic alterations mirror damage to the white matter tracts connecting the thalamus to the parieto-occipital cortices. Consequently, an expanded interpretation of the thalamus L-sign could indicate damage to the posterior thalamocortical connections, potentially manifesting as injuries within both gray and white matter.
Four cases exhibited an asymmetric thalamic L-sign, which was exacerbated by additional white matter injury related to IVH and periventricular hemorrhagic infarction. IVH typically originates from the germinal matrix, and as the germinal matrix bleed enlarges, the underlying ependyma breaks, filling the ventricle with blood. The severity of IVH is graded according to ultrasound findings, with grades ranging from hemorrhage confined to the germinal matrix (grade I) to IVH with acute ventricular dilatation (grade III). Parenchymal echogenicity is often referred to as grade IV IVH; however, such lesions usually represent periventricular hemorrhagic infarction, which results from compression of the medullary veins draining the white matter rather than an intraventricular hemorrhage that extends to the parenchyma. IVH may cause damage to the adjacent white matter, as revealed by autopsy studies showing evidence of white matter injury in 50–80% of infants with IVH [17,18,19,20]. Typical microscopic findings in the periventricular white matter and germinal matrix include scarring and astrogliosis with reactive astrocytes, hemosiderin-laden macrophages, and calcifications [19,20,21]. Periventricular hemorrhagic infarction on the other hand usually evolves into a single porencephalic cyst that communicates with the lateral ventricle or a cluster of periventricular cysts that remain separate from the ventricle. Hemorrhagic necrosis in periventricular hemorrhagic infarction is typically unilateral and asymmetric, resulting in asymmetric white matter injury [20]. Therefore, the presence of an asymmetric thalamic L-sign signifies an asymmetric white matter injury, probably related to additional ipsilateral high-grade IVH. This contrasts with the exaggerated L-sign described in term infants with partially prolonged HII and hypoglycemia, which typically affects the bilateral posterior parieto-occipital cortex and adjacent white matter in a symmetric manner.
Although further studies of the thalamus L-sign with long-term follow-up are warranted, our findings suggest that it may aid in prognostication and serve as a marker for future disabilities, including the development of cerebral palsy. Early identification of the L-sign may therefore facilitate timely, targeted interventions, aligning with current recommendations to begin treatment at the diagnosis of cerebral palsy or high-risk cerebral palsy [22].
From an imaging perspective, radiologists should be familiar with the thalamus L-sign and its significance. Recognizing the L-sign can also help avoid misdiagnoses and irrelevant considerations, such as neurometabolic diseases, thereby improving diagnostic accuracy and patient management.
This study has several limitations that require consideration. First, the limited number of patients in the cohort restricts our ability to further investigate the thalamus L-sign in prematurity, particularly in cases where it is asymmetric (with only four patients in this study). Another limitation of this study is that the images were interpreted in consensus rather than independently. This approach, while ensuring a thorough and comprehensive evaluation, limits the ability to quantify interobserver variability. An additional limitation of our study was that patients were evaluated retrospectively, with a lack of standardized recording of clinical information and inconsistency in the timing and protocols of MRI studies. Furthermore, the absence of advanced MRI techniques, such as diffusion tensor imaging, restricts a comprehensive evaluation of the white matter tracts, which is crucial for gaining thorough neurodiagnostic insights. Finally, the absence of long-term follow-up data hinders our understanding of the prolonged neurocognitive consequences of the thalamus L-sign. Future studies aimed at further exploring the thalamus L-sign could significantly enhance our understanding of this finding. This includes examining the thalamus L-sign in other populations, such as term neonates with white matter injury and PVL. Additionally, future prospective studies with larger cohorts, standardized protocols utilizing advanced techniques, and long-term clinical follow-up could help us further characterize the thalamus L-sign and its clinical significance.

留言 (0)