EBV-positive lymphoproliferative diseases encompass a range of conditions, including both reactive and malignant disorders. In this study, we examined seven patients diagnosed with EBV + T/NK cells in the IM. All patients survived and are currently under long-term clinical observation and follow-up. It is important to recognise this disease and differentiate it from NK/T-cell lymphoma, systemic EBV + T-cell lymphoma in children, and HLH presenting with extensive infection of T and NK cells. It is important to recognise this complication, and the differential diagnoses include NK/T-cell lymphoma, systemic EBV + T-cell lymphoma in childhood, and HLH.
IM is an acute disease, primarily caused by EBV infection, predominantly affecting B cells, although rare cases involve T cells [11] and NK cells. It typically manifests with high fever, pharyngitis, and cervical lymphadenopathy and often resolves spontaneously. Microscopically, lymph nodes show obvious paracortical expansion and focal destruction of the lymph node architecture. The infiltrating cells are heterogeneous and include small and large lymphocytes, immunoblasts, histiocytes, and variable numbers of plasma cells and eosinophils [12]. The histological features of IM are so varied that they are sometimes misdiagnosed as malignant lymphoma, particularly in cases with numerous large immunoblasts. The clinical symptoms and prognosis described in our present cases were similar to those of IM, except for differences in the types of EBV-infected cells and certain morphological characteristics. While there were two reports describing an IM patient with atypical T-cell proliferation in the nasopharynx, most lymphoid cells were also positive for CD2, CD3, CD5, CD7, and without loss of T-cell antigen [8, 9]. In the present case, the clinical manifestations and blood EBV antibody test results of some patients were consistent with IM; however, excessive EBV infection of T/NK cells has raised concerns about lymphoma. The staining of EBNA2 helps determine the type of EBV infection in pathology, thereby avoiding overdiagnosis of lymphoma. In the IM, T and NK cells may occur, and these might even be monoclonal [13].
NK/T-cell lymphoma occurs mostly in adults, is invasive, progresses rapidly, and almost always exhibits an extranodal presentation. The nasal cavity, nasopharynx, paranasal sinuses, and palate are most commonly involved, with the nasal cavity being the prototypic site of involvement [5]. Some cases may also be accompanied by secondary lymph node involvement [14,15,16]. Isolated nodal involvement in NK/T-cell lymphoma is extremely rare, and only a few cases have been described in published work [17,18,19,20,21]. NK/T-cell lymphoma is highly aggressive, with short survival times and poor response to therapy; therefore, the clinical outcomes are dismal. Differentiating between EBV + T/NK cells in IM and NKTL based on morphology and immunophenotype is difficult. However, NK/T-cell lymphoma often lacks systematic clinical manifestations at onset and progresses rapidly, causing significant damage to adjacent tissue structures. At the same time, we observed positive EBER staining in cells of varying sizes in our cases, suggesting that EBV infection affected cells at different stages of differentiation. The self-limiting characteristic of EBV + T/NK cells in IM underscores its clinical significance. When managing such conditions, careful considerations and selection of treatment strategies are paramount.
Systemic EBV + T-lymphoma in children, according to the WHO classification [5] and Category B classification by Ohshima et al. [7], develops shortly after primary or acute EBV infection and is accompanied by an aggressive clinical course and atypical lymphoid cell infiltration, with most reported cases exhibiting a monoclonal pattern of T-cell proliferation, progressing toward multiple organ failure, sepsis, and sudden death [22, 23]. These malignant tumour features overlapped with those of our present cases in terms of clinical manifestations, pathological morphology, immune phenotype, and clone detection; however, the present patients achieved remission or recovered without relapse during long-term clinical observation. A similar group of cases has been reported [24]; however, the patients died quickly, which differs from our study results. The presence of an abnormal karyotype favours neoplastic conditions and is helpful in identifying systemic EBV + T-lymphoma in children [25]. In the present case, karyotype testing of the three patients showed no abnormalities. The response to HLH treatment is one of the most important parameters for distinguishing IM to Systemic EBV + T-cell lymphoma in childhood.
In the present cases, four patients mimicked EBV-associated HLH, which was described as young age and EBV + T/NK cell proliferation with variable clinical findings, including high fever and splenomegaly, cytopenia, and liver dysfunction, and was accompanied by histological evidence of hemophagocytosis, which causes extremely high serum levels of ferritin, lactate dehydrogenase, and soluble CD25, serological tests, or the detection of EBV DNA or RNA from tissues [26]. After anti-HLH treatment, 4 patients achieved complete remission. The other three patients did not exhibit HLH. In addition to observation and follow-up, symptom relief was achieved without any special treatment. EBV-associated hemophagocytic lymphohistiocytosis (HLH), a hyperinflammatory syndrome induced by a dysregulated immune reaction secondary to EBV infection, is difficult to differentiate in childhood. Clonal EBV-infected T cells have been demonstrated in some cases [13], and patients typically respond to treatment, which can be limited in some cases, with complete recovery following acute disease. Therefore, EBV + T/NK cells in IM can be considered a clinical manifestation of HLH, and the prognosis is generally good after treatment.
Primary EBV-positive nodal T-cell or NK-cell lymphomas have been reported [5, 20, 27]. These lymphomas typically present with lymphadenopathy with or without extranodal involvement, advanced-stage disease, and B symptoms. They exhibit a monomorphic pattern of infiltration and lack of angiodestruction and necrosis seen in extranodal NK/T-cell lymphomas. They are more common in elderly patients or patients with immune deficiency and have a dismal prognosis. Although its immunophenotype is similar to that of EBV + T/NK cells in the IM, it often occurs in the lymph nodes. However, it is more common in elderly patients and has a poor prognosis, which differs from the present case.
It should be noted that a positive monoclonal population does not necessarily predict malignant behaviour because similar populations can be observed under reactive conditions [28,29,30,31]. We identified a clonal T-cell population in four cases (cases 1, 2, 5, and 6). Clonality does not necessarily indicate malignancy, and our results showed that monoclonal T-cell populations are visible in patients with primary EBV infection, consistent with previous reports [13]. Furthermore, the prevention of serious complications such as multiple organ failure, hemophagocytic syndrome, disseminated intravascular coagulation, and sepsis is very important.
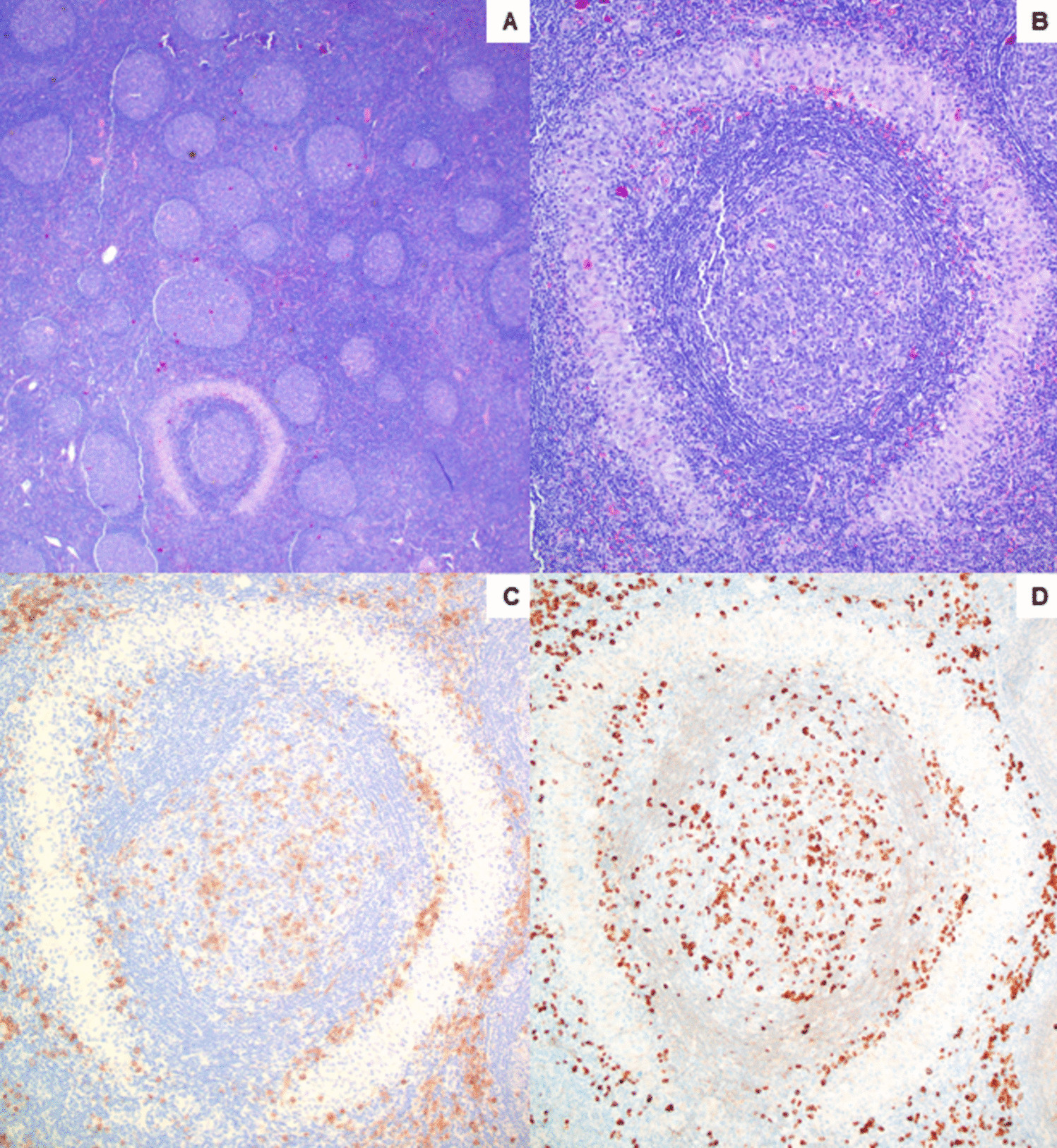
It is pertinent to perform a detailed laboratory examination of either EBV load in the serum or expression of EBV in situ to evaluate cases with a sudden onset course. In the present case, serological studies were incomplete or had not been performed. EBV-CA-IgM positivity was observed in three patients (patients 1, 2, and 7), EBV-CA-IgG positivity was observed in six patients, and six patients showed increased EBV DNA. EBV serology in such cases may be clinically misleading, as it may not conclusively indicate acute primary or active infection. However, the precipitous onset of symptoms in previously healthy young individuals is along with biopsy samples showing infiltration of numerous EBER-positive and scattered EBNA2-positive cells suggesting an acute process. In particular, CD8-positive cells increased, suggesting primary EBV infection. EBNA2 (Epstein-Barr virus nuclear antigens 2) is a gene product expressed during latent EBV infection. As a key transcription factor, it regulates the expression of viruses and many genes in cells during viral infection of lymphocytes [11]. Furthermore, EBNA-2 was expressed in four cases with scattered positive nuclei, three of which had increased anti-EBV VCA IgM antibodies. EBNA2 is a useful marker expressed in patients who have a primary immune response or are immunocompromised; IM patients usually have EBNA2-positive cells [9]. Additionally, in the present cases, the indices of liver function and other markers of illness severity in EBV infection were either incomplete or had not been evaluated previously. Therefore, patients with a high viral load in their blood and particularly intense expression of EBV in their vital organs require more intense clinical supervision.
EBV + T/NK cells in the IM can elicit both pathologically malignant and clinically benign features. Thus, detailed clinical information including age at onset (children and young people), nature of onset (sudden), disease course (short), symptoms (systemic), EBV infection status (acute), and lymph node involvement is crucial for the diagnosis and prognostic evaluation of this disease.










留言 (0)