
記住我
Dear Editor,
Pigmented papular lesions can have varied differentials, especially in skin of colour, including seborrheic keratosis, melanocytic naevus, dermatofibroma, leiomyoma, pigmented skin tag, pigmented poroma, nevoid basal cell carcinoma, pigmented trichoblastoma and others. Besides, the face is a relatively common location for verruca plana, milia and syringoma; the last two entities can have pigmented morphology in the skin of colour.
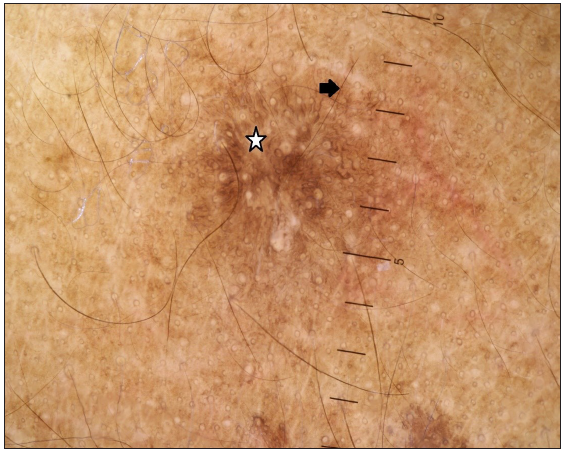
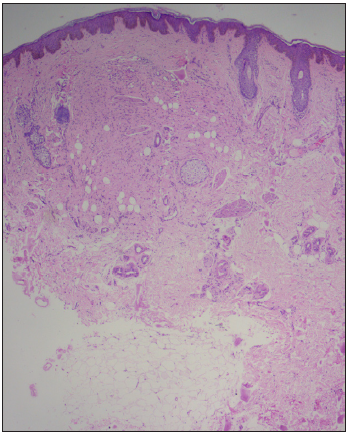
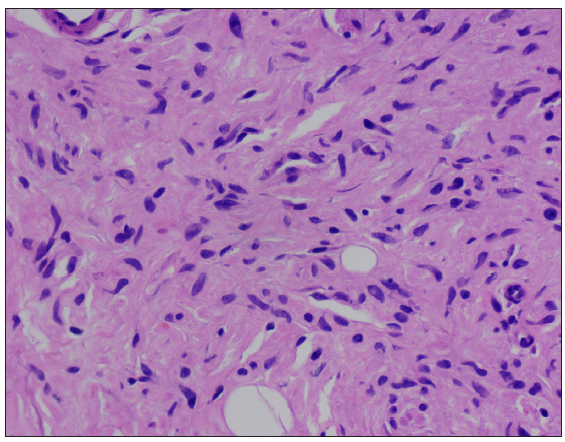
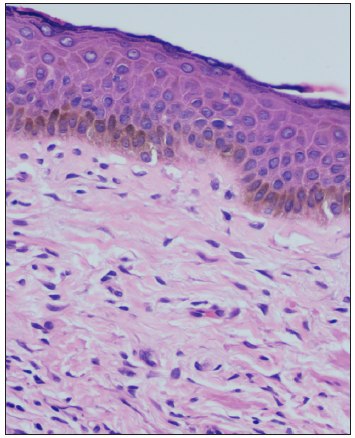
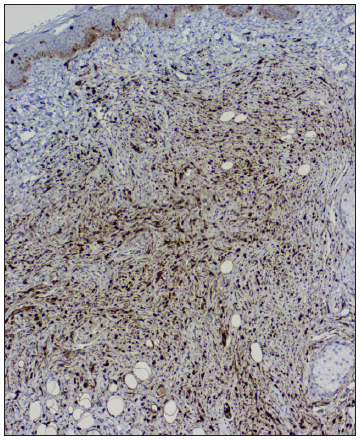
A 55-year-old female presented with multiple mildly itchy skin lesions over her right cheek for two years. On examination, multiple monomorphic, brown, dome-shaped, 2–5 mm sessile papules were noted on the right cheek [Figure 1a]. Dermoscopy revealed fingerprint-like structures on a background of a brown homogeneous area [Figure 1b]. There was no evidence of freckles or café au lait macules (CALM) and the button-hole sign was negative. Systemic and mucocutaneous examinations were normal. The possibility of pigmented syringoma, pigmented trichoepithelioma and pigmented milia were considered. Histopathology showed epidermal hyperpigmentation with a non-encapsulated dermal tumour composed of short spindle-shaped cells with wavy s-shaped nuclei [Figures 2a-c] with immunohistochemistry revealing diffuse positivity for S-100 [Figure 2d] and negative for HMB45. The epidermis had increased melanin in the basal and suprabasal layers. A diagnosis of neurofibroma (NF) was considered, and a detailed evaluation for any syndromic association yielded negative results.

Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
NF is a benign tumour and originates from a nerve sheath. Multiple NF associated with CALM and freckles are not difficult to diagnose; however, the solitary form or non-syndromic NF can be a diagnostic challenge. Pigmented NF is a rare entity that constitutes less than 1% of all NF, and it presents as solitary or multiple pigmented papules or nodules predominantly over the scalp, usually in the second or third decade. In addition, pigmented NF acquires a brown colour, either due to the increase in epidermal melanin or pigment deposition in between tumour cells, requiring it to be excluded from other pigmented skin papules.1 Our case was unique due to the arrangement of the pigment papules in an agminate fashion. The dermoscopic features of syndromic NF are a peripheral pigment network (regular or irregular brown network extending beyond the borders of the lesion); a peripheral halo of brown homogeneous pigmentation (continuous or discontinuous dark or light brown homogeneous pigmentation at the borders); fingerprint-like structures (brown, fine, parallel cord-like structures); pink-red structureless areas (pink to red areas); fissures (irregular linear crypts); and scar-like areas (opaque white distinct areas).1
The agminate arrangements of facial papules are described in the literature in blue naevus, spitz naevus and colloid milia. Agminate blue naevi present as blue clustered dome-shaped papules at birth or the second decade. Dermoscopy reveals homogeneous blue or blue-black pigmented structures. Histopathology shows pigmented dendritic bipolar spindle melanocytes admixed with melanophages in the superficial dermis with melan A and HMB-45 positivity.2 Agminate spitz naevi present as grouped, pink to brown, dome-shaped papules and nodules over the face and trunk in the second decade. Biopsy demonstrates naevus cells embedded in a desmoplastic stroma diffusely in the dermis with little junctional activity, and dermoscopy showing a starburst pattern with reticular depigmentation.3
Cells of neural, muscle, histiocytes, fibroblasts and endothelial origin have spindle cell morphology. Smooth muscle cells have deep eosinophilic cytoplasm with a thick cigar-shaped, round-ended nucleus with positivity to smooth muscle actin and vimentin, fibroblasts show less eosinophilic cytoplasm with nuclei with tapered ends,while neural tissue has pale eosinophilic bubblegum cytoplasm with wavy nuclei with S100 positivity. Facial papules with spindle cell morphology are described in neurotised congenital melanocytic naevi (NCMN), fibrous papules, eruptive collagenoma, desmoplastic cellular neurothekeoma (DCN), dermatofibroma and trichodiscoma.
NCMN and pigmented NF pose diagnostic challenges as both have a neural crest cell origin. On histopathology, prominent clustering of melanocytes in cords and nests with S100, Melan A and HMB 45 positivity is described in NCMN.4 DCN on histopathology shows nests and cords of bland epithelioid to spindle cells with myxoid and dense fibrotic collagenous stroma with IHC negativity for S100, positive for S100A6, CD 63 and PGP 9.5.4 Biopsy of fibrous papules shows dermal proliferation of stellate fibroblasts with collagen arranged concentrically around hair follicles and blood vessels with thin-walled dilated vasculature.5 Multiple clustered dermatofibroma on histopathology reveal a hyperpigmented basal layer, Grenz zone, spindle-shaped fibrous cells admixed with histiocytoid cells and IHC shows factor XIIIa and CD68 positivity.6 Trichodiscomas are fibrovascular hamartoma of hair disks that shows proliferative connective tissue with anastomosing strands of follicular epithelium on biopsy.7
We are reporting this case due to the rarity of pigmented, non-syndromic variant of NF, with a unique arrangement in agminate fashion, where dermoscopic and histopathological features aid in arriving at the diagnosis.
留言 (0)