
記住我






Borderline Personality Disorder (referred to as “BPD” hereinafter) is a severe mental disorder, which can be observed in various intensities and manifestations, both clinical and sub-clinical, characterized by some pathognomonic elements: emotional dysregulation, impulsivity, difficulties in interpersonal relationships and chronic feeling of emptiness (Chapman 2019) which, in most cases, around 79% of them, is linked to a deep fear of abandonment and rejection (Luyten 2019). We observe, then, that this personality disorder is based on a generalized destabilization, which attacks various levels of the person: from their intrapersonal image to their external relationships (always by virtue of an uncontrolled, disordered, figureless interiority).
Many studies have been dedicated to the etiology of this and all personality disorders, finding, in the case of BPD, an important association: the introjection of victim-victimizer roles in contexts of violence, whether physical, sexual or psychological (Stith et al. 2020). These roles are essential because, from a systemic perspective, they delimit the way in which the diagnosed individual relates not only to the world around him, but also to himself, which is of vital importance for this article; which focuses, among other topics, on the development of BPD within the framework of a life history marked by sexual abuse. There is a significant relationship between this type of violence, which is based on force, manipulation, coertions, or use of threats to get a child to participate in sexual relations with the perpetrator (Caballero et al. 2024), either through touching the sexual act itself, or even by forcing them to watch pornographic content (Save the Children 2018) and the subsequent appearance of BPD, especially when the perpetrator is a man and the victim is a woman (Mainali et al. 2020).
The consequences of sexual abuse in childhood in its various manifestations have been the subject of constant study in child psychology, with special interest in the development of personality and attachment styles (Ahn et al. 2022; Khanjani et al. 2023). Researchers such as Tingtin et al. 2021) have tried to systematize the consequences of sexual abuse in childhood, and found that there is, mainly, a deep discomfort and a dysphoric emotional state that remains constant in the life of abused children, manifested explosively as abreaction at different times in situations that are unconsciously associated with the abuse or with the figure of the abuser. Thanks to this information, it is possible to conclude that a significant part of the patient’s psyche remains fixated in this event, at least on an unconscious level. Said consequences are not limited only to the psychological and physical aspects, but also the physiological, neurological, social, and even spiritual aspects (Letkiewicz et al. 2020). This can be deeply related to the possibility to form personality disorders and intense modifications in the victim’s behavior throughout their life (Bounoua & Sadeh 2022), such as emotional dysregulation, depression and reductions in empowerment and self-confidence, so it is safe to say there is an important relation between traumatic events such as sexual abuse and the intrapersonal experience, mainly affecting not only the relationship with one’s own body and one’s own sexuality (Gewirtz-Meydan et al. 2023), but also attachment styles and tools to form interpersonal relationships (Hashworth et al. 2021).
Likewise, in said investigation, it was observed that the surviving participants of sexual abuse had fewer psychological resources to face the difficulties of daily life, a greater dependency on their interpersonal relationships, and anxious and/or ambivalent attachment styles (Hashworth et al. 2021; Tingtin et al. 2021). This is consistent with other studies, which conclude that 44% of people who suffered sexual abuse during their childhood develop a BPD (Menon et al. 2016). An important element to take into consideration is the attachment styles that these types of patients handle, oscillating between anxious and ambivalent styles. It has been demonstrated in the case of this particular personality disorder that there is an important fixation on the occurrence of trauma that stops the possibility of relating adequately with the world, of establishing links through emotional containment and to manage and understand their own emotions. In this case the systemic approach is proposed as a framework, which aims to restructure interpersonal ties and understand them in terms of roles (sometimes conscious or unconscious) that align with the appearance of symptoms. (Porter et al. 2019). This perspective enables the possibility of intervening in the particular characteristics of the clinical case to be discussed in relation to the occurrence of sexual abuse, parental triangulations, and the couple’s relationship. This anachronism is a perspective that allows us to understand the linearity of the disorder and, therefore, its etiology.
The literature on possible treatments for this type of case is extensive and highly scientifically valid, as we observe in the case of mentalization, dialectical behaviour therapy, emotion regulation group therapy, and many more, (Arntz et al. 2023; Lorenzini 2021), with great results in terms of effectiveness, adaptation to the society, decrease in suicidal ideation and chronic feeling of emptiness. Every intervention carried out in the present clinical case, although structured from a systemic perspective, includes interventions focused on trauma with techniques such as mentalization and emotional regulation, achieving significant results in relation to the feeling of well-being expressed by the patient after her therapeutic process.
Recognition of one’s own and third-party mental processes was prioritized at all times, so as to empathize, understand, and self-regulate in favor of an adequate emotional bond, as suggested by Fonagy (2017) and (Martin-Gagnon et al. 2023), with a focus on movements at the role level not only in the life of the patient and her family, but also the roles that are manifested during consultations.
As stated, a brief clinical case will be presented below that clearly illustrates the phenomena mentioned above. Much information has been limited for reasons of length, so only vital data will be presented.
Clinical CaseThe patient is a 33-year-old woman who will be identified from now on as “Sofia”, attends the consultation due to a series of dysphoric symptoms related to a BPD that, although they were present throughout her life, increased in magnitude after intrapersonal conflicts with her partner (named as “Giovanni) and the possibility of being abandoned appeared in her life. Relevant precedents such as episodes of sexual abuse, incest, and hypersexuality during adolescence and early adulthood will also be evidenced, as well as serious interpersonal difficulties with the members of the family nucleus, especially her mother. The patient currently lives in Switzerland with her husband and a two-years old son.
First Contact with the PatientSofia arrives at the office for the first time in a visibly anxious state, showing great psychomotor agitation. She expresses that this is common for her when alone with men, saying that she doesn’t quite understand why, which is very common in victims of sexual abuse perpetrated by masculine figures. From the beginning, it is vital to establish a positive therapeutic alliance that functions as an initial framework to build the patient’s recovery (Barros 2023).
THERAPIST: I can see that you are very agitated, Sofia. Your legs and hands are moving quickly. What are you feeling? Is there something going on?
SOFIA: I don’t know, actually. I don’t feel very comfortable being alone with men. When I was little, I… well, I don’t know. It’s nothing. I don’t know what’s happening to me. Please, don’t think that I don’t want to be here, I want you to help me. I feel like I’m going crazy. I need to get better for my family. If I lose them, I don’t know what would I do….
THERAPIST: Sofia, don’t worry. There are things we’ll discuss when the time comes, at your own pace. I don’t expect you to tell me everything in the first session. I want us to build a relationship of trust, for you to know that I’m here for you. Okay?
Upon delving deeper into her stated reason for seeking therapy, we find that infidelity on her partner’s side triggered a spiral of emotions accumulated for years that has been obsessively weighing on her ever since.
THERAPIST: Sofia, I sense that you greatly fear losing your marriage and family. I would like you to tell me for how long you have felt this way and why you feel this is a real danger. (SOFIA remains silent for a few minutes, fixing her eyes on the ground. She rubs her hands.)
SOFIA: I have always felt this fear—I have always been afraid that one day he will wake up and no longer want to be with me. But two weeks ago, I found out what happened. A horrible event. He betrayed me. He did what everyone has done to me all my life. My dream of having a perfect family was destroyed.
THERAPIST: Do you want to tell me what happened?
SOFIA: Yes, yes… He cheated on me with his coworker. He slept with her. I was getting better, everything was going well, and I was beginning to forget my past. And now this happens.
Sofia bravely admits that her goals are “to form a family with Giovanni, to be happy, to fix it,” so her expectations for the psychotherapeutic process initially rely on “getting better” due to a marked fear of losing her current partner, who has been an “indispensable pillar” to “maintain her sanity in her internal madness”.
SOFIA: I feel empty inside. I don’t understand why he did this to me when I’ve given him everything.
THERAPIST: What are your expectations with this process that we are starting together?
SOFIA: I want to forgive him, but he has to admit his mistake and promise me he won’t cheat on me again. I want us to be a happy family again. He is my light, he is my everything.
This difficulty in self-nomination is characteristic of BPD, and is classified within the pattern of instability found not only in Sofia but in many other cases. This intrapersonal instability has been, in the patient’s words, a constant in her life in different contexts: from the difficulty of keeping a job, to maintaining a partner without resorting to manipulation through suicidal intention. The systemic approach, whose method consists of the contextualization of the symptom in the framework of interpersonal relationships (Giordani et al. 2016), allows us to understand this symptomatological manifestation together with Sofia’s life and history. Throughout the sessions, Sofia recognizes a “big black gap” in her history, tracing it back to a cardinal fact: maternal and paternal impositions. “My desire was postponed to desire what others wanted from me,” Sofia concluded.
The work methodology, then, consisted of free association, allowing the free flow of ideas and their subsequent association to the central aspects of the patient’s condition: interpersonal problems, suicidal attempts, polarizing and egodystonic cognitions. Through this association, extremely valuable findings were made regarding the patient’s biographical history, thus establishing thematic pillars that were ordered according to their priority (suicidal ideation, conception of death, abandonment, sexuality), all related in similar proportions to the relationships with her mother and father, as well as with the traumatic event of abuse.
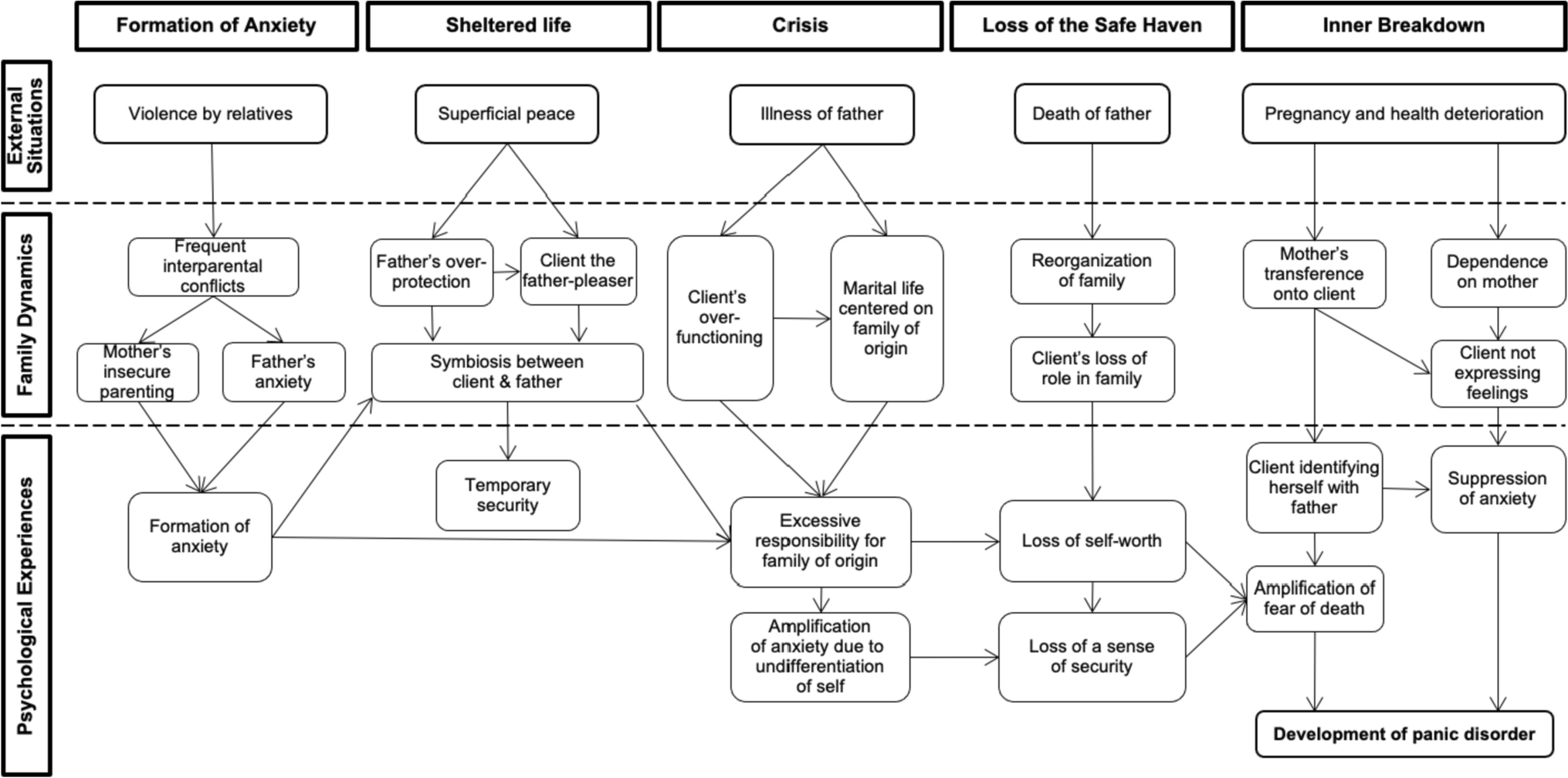
About her Childhood and Family RelationshipsIn reference to how Sofia’s family is structured, see Fig. 1.
SOFIA: It’s very difficult to talk about my father. He touched me. He would come into my room at night and sit next to me. He would sit me on his lap since I was little. He eventually stopped when he got really sick and lost most of his mobility. I was a teenager then. I told my mother several times what was happening, but she never believed me. She called me a whore, and told me not to make up lies, to shut up. It hurts to think that she knew but never did anything to stop it. He was very violent with everyone. My mother was too, but when
Her mother, an aggressive, emotionally cold, and hostile woman at all times, would talk to her about her refusal to breastfeed her when she was a newborn baby, and how she would “abandon” her in her room at night despite her cries. When exploring the possible consequences of years of chronic abuse, Sofia recognizes firstly that said “black lagoon” (referring to a clouding of consciousness) in her mind is mainly related to the fact that she has never lived a truly spontaneous, meaningful life. From a systemic approach, it was possible to observe how the roles developed at home, as well as the interpersonal relationships between mother-daughter and father-daughter, contributed significantly to this psychological arrest: reducing trust, individuality and internal resources (Dallos et al. 2021). For Sofia, the roles played by her parents towards her resulted in a “psychic introversion” (in the sense of an “inward escape”) that remained throughout her childhood, adolescence and part of her adulthood. For Sofia, everything was projection: projecting the roles learned in her parent-child relationship (victim-abuser, dominator-dominated, who abandons-who waits) in the majority of her significant relationships, prioritizing the desire of others instead of her own, as a form of external locus of control.
This combination is significant in the construction of one’s own sexuality (Krause-Utz 2021). Sofia recognizes that sexuality and compulsive seduction have been part of her life since the first instances of abuse: behaviors aimed at stimulating the male figure, with significant ambivalence as she expressed opposite and polarizing fantasies of caring and killing, retaining and fleeing. She describes men as “evil, manipulative, deceitful, and treacherous,” mainly remembering her father.
At 14 years old, she had her first sexual experience with a 24-year-old man who lived in her neighborhood. From then on, she developed a compulsive attitude towards sexuality, until she met Giovanni. In this case, we could suppose that the compulsive manifestation of sexuality after abuse can be an expressed symptom to lessen anxious stimuli (Fontanesi et al. 2021), especially when the individual makes a conscious effort to suppress the traumatic experience, coupled with the relational background that contextualizes the symptom.
Symptomatology and PsychodiagnosisRegarding suicidal ideation and episodes of anxiety and depression, the decision was made to apply the Beck Depression Inventory (BDI-II). Its objective is to evaluate, briefly and concisely, the existence and the severity of depressive symptoms in the patient. As a result, a score of 51 was obtained, which is categorized as “severe depression,” demonstrating that the patient shows severe episodes of depression without the presence of pathognomonic positive symptoms of psychosis. Only the aforementioned inventory was applied mainly for reasons of time, and only with the objective of confirming the severity of depressive symptoms.
Taking into consideration the symptoms presented during the psychotherapeutic process, as well as the relational patterns and attachment style displayed, borderline personality disorder (DSM-5 301.83; ICD-10 F60.3) is assigned as the nosological entity, with notable comorbidity with a specified depressive disorder (DSM-5 311; F32.8) as the necessary criteria for diagnosis are met, namely: a pattern of instability that persists in interpersonal relationships, emotions, and body image; pronounced impulsivity; significant difficulty in tolerating loneliness; self-mutilation, suicidal ideation and attempts on repeated occasions; persistent sense of emptiness; dissociation in response to stress; a troubled relationship with one’s sexuality (American Psychiatric Association, 2013).
Therapeutic ProgressFrom the beginning, the most affected areas in Sofia’s life were her intrapersonal life, her family life, and her work life, all permeated by a generalized loneliness, a feeling of isolation, and a distrust of everyone around her. Thus, thoughts associated with inflexibility, over-generalization, catastrophic vision, personalization and polarized thinking were evident.
Likewise, Sofia managed to identify an important association between her hypersexuality and a repressed hostility towards men: two sides of the same coin. This was of great interest for the therapeutic process, since, as has been observed in different investigations (Martin-Gagnon et al. 2023), the sexual instinct (primarily associated with what we call “what the other wants”) was in contrast to one’s own desire, progressively resulting not only in the destruction of the image of the other through conflicts, but also in self-destruction expressed in growing suicidal ideation.
Through the therapeutic process we were able to identify that interpersonal conflicts, that is, those that were generated between her and the surrounding world, resulted mainly from projections, from an internal world to which she compulsively clung in order to make sense of an external world that did not exist. She was able to understand, in the absence of resources, what mentalization can be like.
The systemic approach provided not only the framework to understand that the nature of these projections was, primarily, relational in the sense that it was progressively formed from patterns inherent to family dynamics (Zeifman et al. 2021), but also the idea that all the symptoms that Sofia experienced with pain were a kind of internal call to wake up and visualize everything that was happening inside her, opposing the blinded and thoughtless way with which she experienced the phenomena of the world.
SOFIA: Yes, I really don’t want to talk about her (her mother). You know, the truth is that the issue of abuse with my father is something that I have been able to cope more easily, but the fact that my mother was never there for me and turned her back on me when I needed her the most is something that breaks me inside.
From the mother-daughter bond, and the rejection of the maternal image, a disconnection from Sofia’s feminine aspects occurred. This led to difficulties in raising her son, rejecting him and distancing herself from him, as well as sexual conflicts with her partner. Once we became aware of this fact, we could begin to cognitively restructure the associations (or projections, rather) that came from the internal world, towards external phenomena, seeking a kind of “psychic objectivity”, if you will.
The different techniques used for the intervention, such as mentalization, were part of the risk management plan (Hawton et al. 2022), which consisted mainly of the following elements: (1) strengthening community and family ties; (2) active participation in a Christian church meant very valuable support for the patient; (3) restricting access to materials that could lead to suicide (i.e. keeping knives and toxic chemicals away); (4) the development of a concise life project in accordance with the patient’s wishes, which were previously largely repressed; (5) the frequency of meetings was increased, with the aim of providing containment, especially during depressive episodes. The inclusion of her husband in this plan proved to be extremely effective.
On the other hand, it should be mentioned that the therapeutic relationship plays an indispensable role in the healing process, especially in patients whose attachment styles have not developed in the neutrality of a secure base. This is the case with Sofia, who, from the moment she was born, was systematically denied by her mother, who refused to breastfeed, care for, and protect her; and sexually, physically, and psychologically abused by her biological father, fragmenting her weakened psychic system to the point of seriously hindering the formation of a solid identity.
Although the pertinent legal actions against her father were never taken, initially due to the patient’s fear, complicity of the mother, and later due to the death of her father, the patient decided as a result of the therapeutic process that, beyond the lack of said legal measures - however necessary they may have been -, she would take charge of her destiny and her life. This corresponded with an important insight during the first four sessions.
As the center of therapeutic action, as is well known in the systemic model, the psychotherapist must maintain a “close distance” from an empathetic perspective, in relation to the patient and the image of their family, achieving integration between the patient’s relational needs and the characteristics of their family nucleus. In this sense, the sure step as a psychotherapist consisted of becoming a secure base of support, empathetic accompaniment, reflecting the patient’s affective deficiencies when they appeared in her discourse, making them visible, and responding to them without distancing oneself from the professional role.
SOFIA: I have talked to you about my mother’s gaze. She used to look at me with hate and resentment, as if I had taken away a part of her life. For most of my life, I felt motherless. With you, I have remembered all the people who have looked at me with love, not only my husband and my son but also my friends and my brother, who has always been there for me.
Although Sofia was initially evasive, distant, and distrustful of the therapeutic process, as is common in patients with her diagnosis (Folmo et al., 2021), it was possible to build a therapeutic process in which she gradually confronted the etiology of her symptoms. Perhaps the most complex step in patients with similar biographies is the full recognition of the harm caused by the perpetrators, not only at the level of physical integrity but also at the psychological level. One of Sofia’s biggest difficulties was recognizing her traumatic event as the catalyst for the symptoms that constantly plagued her: nightmares, compulsive sexuality, the pursuit of perfection, passive suicide attempts, and fear of loneliness.
Overcoming repression involved, for Sofia, recognizing herself as a truly vulnerable, self-conscious, distant, and weakened person in the face of the circumstances of her life. In this process, the psychotherapist served as a mirror, returning through his gestures, facial expressions, and words the sensations that Sofia had effectively repressed as a defense mechanism, absolving herself of the episode of sexual abuse.
SOFIA: My mother and father repeatedly told me that everything bad that happened to me was because I brought it upon myself. If I was beaten at home, it was because my behavior was not good enough; if I was forced to fulfill all the responsibilities of the household, it was because I spent too much time with my friends. There was always a justification for all the abuse.
THERAPIST: And the hardest part of it all is that these justifications were internalized, and you believed them yourself, to the point that, in your adult life, you still tried to justify all your suffering. This makes it impossible to take responsibility for our own process, don’t you think?
SOFIA: Yes, that’s right, doctor. You are right.
A significant part of the psychotherapeutic work and efforts were directed not only towards creating awareness about the causes and reasons for suffering but also towards learning to live with it and finding the treasure of learning in that darkness, freeing oneself from the burden of self-blame. One of the most powerful phrases that Sofia uttered during her therapeutic process was: “I feel that I am the sum of everything I have lived”; there lies the imperative recognition of being oneself, a strengthening of the psychic system where not only one’s identity and self-image are reinforced (such important elements for Sofia in her suffering), but also the timely validation of emotions that she spent so much time keeping secret.
A significant breakthrough is related to the re-signification of some particular symptoms and events from early childhood. Among them, we can highlight the “solitude-suicidal thoughts duality,” as named by the patient, where it was identified that every crisis that occurs in the context of abandonment or in the face of the possibility of being alone arises as an autonomous response related to the traumatic event (which represents a helplessness episode) and the need to be rescued. This level of awareness allows the patient to develop a more realistic sense of responsibility for her emotions and herself, as well as facilitating the development of mentalization. Mentalization, coupled with a systemic approach that comprehends the deep roots of the patient’s suffering has proven to be very useful (Rask, 2019) to generate internal tools that allow emotions to be regulated, understood, and contextualized.
SOFIA: That thing you said about living in guilt being a form of narcissism also… It impressed me. I hadn’t seen it that way.
THERAPIST: It’s similar to living with a mirror in front of you all the time. A mirror that blames you for everything and doesn’t allow you to look beyond your own negative reflection, a mirror that reflects those black spots.
SOFIA: Yes, it’s a defense mechanism, as you call it. (SOFIA laughs.) The truth is that I had never seen it so clearly. My childhood was very difficult, but the rest of my life didn’t have to be like that; in fact, it hasn’t been as hard as I thought. I know that now everything is in my hands and that I must make an effort to be aware of these attitudes.
留言 (0)