
記住我



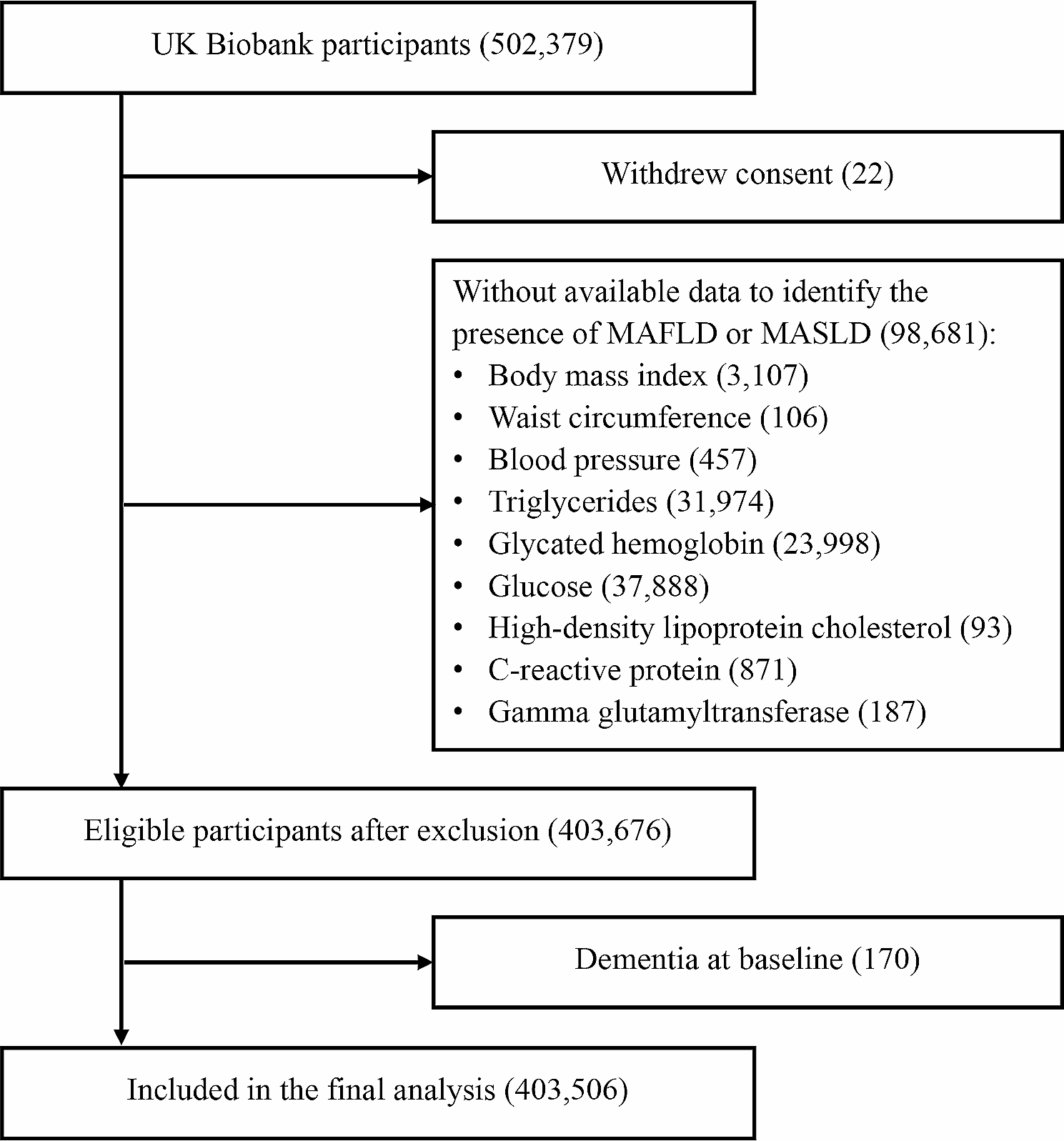


According to before mentioned search strategy, 1148 published studies were identifies from the selected database. Fifty-nine studies were retrieved after screening titles and abstracts. Forty-one studies were excluded due to study design (n = 37; 1 review, 9 study protocols, 22 conference abstracts, 1 participants aged < 60 years, 4 non-randomized controlled studies), full texts not available (n = 4). Three additional studies were excluded as complete data was not obtained from the articles or authors. Finally, 15 studies with 685 patients met the eligibility criteria (Fig. 1). Patients demographic characteristics were found in Table 1. Mean age of patients included studies ranged between 69.0 and 76.6 years old, and education years of most patients had mean over 6 years except 2 studies [18, 28]. For pre-treatment cognitive assessment, Lu et al. [29] used ADAS-Cog, Gonzalez et al. [30] used MoCA, and the others used MMSE.
Fig. 1 Table 1 Patients demographic characteristics of included studies in this reviewStudy characteristics
Table 1 Patients demographic characteristics of included studies in this reviewStudy characteristicsDetails of 15 included studies were summarized in Table 2. Studies included in this meta-analysis were published between 2013 and 2022. Among those studies, 9 used tDCS as intervention of NIBS [18, 28,29,30,31,32,33,34,35], another 6 used rTMS [17, 36,37,38,39,40]. Two studies used randomized cross-over design [34, 35], the others used randomized controlled design. For target patients, 4 studies included MCI [29, 30, 32, 35], 9 studies included AD or other dementia [17, 18, 28, 33, 34, 36,37,38, 40], and 2 studies included both AD and MCI [31, 39]. For tDCS stimulation montage, anodal tDCS F3 montage [28, 30,31,32,33] was utilized in half studies, while other studies utilized anodal tDCS T3 montage [29], P3 montage [34], and T6 montage [35], respectively. Only 1 study chose multisite anodal tDCS montages including F3, F4, F5, P4, P5 and CP5 [18]. For stimulation montage of rTMS, 5 studies utilized multisite montages [17, 36,37,38, 40], except 1 study used F3 montage [39]. Most of studeis administered NIBS stimulation and CT simultaneously, except 1 studies administered tDCS earlier than CT [32] and 1 study administered rTMS earlier than CT [40]. We obtained follow-up data from 11 studies, while 2 studies were unable to be included in results analysis due to missing follow-up data [37, 38]. Two studies did not include follow-up assessments in their methodology [18, 35].
Table 2 Study characteristics in this reviewRisk of bias assessmentThe PEDro scores ranged from 6 to 9, with a median of 7.9, indicating that the methodological quality of included studies was relatively high. All included studies were classified with “Excellent” or “Good” quality, reporting adequately with regard to their “random allocation” and “blind subjects”. However, no studies satisfied the “blind therapists” criteria. A detailed evaluation of PEDro scores was shown in Table 3. In risk of bias assessments, 4 studies were found to have high potential risk of bias because of insufficient concealing group allocation for patients or no fully reporting primary outcomes [28, 33,34,35]. Risk of bias assessments with included studies in this review were shown in Figs. 2 and 3.
Table 3 PEDro assessment quality results in this reviewFig. 2
Risk of bias graph according to the Cochrane risk of bias tool
Fig. 3
Risk of bias summary according to the Cochrane risk of bias tool: “ + ”, “-” and “?” respectively indicate low, high, and unclear risk of bias
Meta-analysis resultsDue to the limited or absent data available of rTMS combined with CT studies on specific cognitive domains, we conducted separate meta-analysis for specific cognitive domain in tDCS combined with CT studies. Only subgroup analysis was performed exploring both tDCS and rTMS on global cognition. In this review, cognitive domains were analyzed including global cognition, executive function, attention/working memory, memory, and language. Cognitive domains and outcome measures for each study were shown in Table 4.
Table 4 Cognitive domains and outcome measuresEffects of NIBS combined with CT on different cognitive domainsTotal of 12 studies with 591 patients reported global cognition scores including 6 studies performing tDCS combined with CT (n = 375) and 6 studies performing rTMS combined with CT (n = 216). The result of meta-analysis showed that NIBS combined with CT significantly improved global cognition scores in AD and MCI (SMD = 0.52, 95% CI (0.18, 0.87), p = 0.003; Fig. 4A). In subgroup data analyses, rTMS combined with CT significantly improved global cognition scores in AD and MCI (SMD = 0.46, 95% CI (0.14, 0.78), p = 0.005; Fig. 4A), while tDCS combined with CT showed no statistically significant effect on global cognition in AD and MCI (SMD = 0.58, 95% CI (-0.06, 1.21), p = 0.08; Fig. 4A).
Fig. 4
Meta-analysis of NIBS combined with CT on different cognitive domains (A-E)
For meta-analysis of specific cognitive domains, only studies involving tDCS combined with CT reported the results of specific cognitive domains scores. Three studies with 245 patients showed that tDCS combined with CT improved language scores compare to the control group (SMD = 0.29, 95% CI (0.03, 0.55), p = 0.03; Fig. 4E). However, the pooled results of 4 studies with 138 patients on execution function (SMD = 0.02, 95% CI (-0.35, 0.39), p = 0.92, Fig. 4B), 6 studies with 407 patients on attention/working memory (SMD = -0.02, 95% CI (-0.2, 0.18), p = 0.81, Fig. 4C), 6 studies with 418 patients on memory (SMD = 0.13, 95% CI (-0.07, 0.33), p = 0.21, Fig. 4D) all showed no statistically improvement.
Effects of NIBS combined with CT in patients with different diagnosisThree studies with 315 patients and 5 studies with 382 patients reported attention/working memory and memory scores in MCI, respectively. However, there was no statistically effect of NIBS combined with CT on attention/working memory (SMD = 0.13, 95% CI (-0.51, 0.24), p = 0.50; Fig. 5A) or memory scores (SMD = 0.11, 95% CI (-0.10, 0.32), p = 0.31; Fig. 5B).
Fig. 5
Meta-analysis of NIBS combined with CT on cognitive domains in patients with different diagnosis (A-E)
Eight studies with 246 patients reported global cognition scores in AD. The result showed that NIBS combined with CT was statistically significant improvement on global cognition scores in AD (SMD = 0.77, 95% CI (0.19, 1.35), p = 0.01; Fig. 5C). However, the pooled results of 3 studies with 72 patients did not identify a statistically significant improve attention/working memory (SMD = 0.63, 95% CI (-0.31, 1.57), p = 0.19; Fig. 5D) or language scores (SMD = 0.27, 95% CI (-0.19, 0.74), p = 0.25; Fig. 5E) in AD.
Effects of NIBS combined with CT on follow-upA total of 9 studies with 477 patients reported follow-up global cognition including 5 studies performing tDCS combined with CT (n = 339) and 4 studies performing rTMS combined with CT (n = 138). The result showed that there were no statistically global cognition improvement on follow-upin AD and MCI (SMD = 0.24, 95% CI (-0.02, 0.49), p = 0.07, Fig. 6A). While the result of subgroup analysis showed AD and MCI achieved signifcant follow-upglobal cognition improvement in rTMS combined with CT group (SMD = 0.55, 95% CI (0.09, 1.02), p = 0.02, Fig. 6A).
Fig. 6
Meta-analysis of NIBS combined with CT on follow-up (A-E)
Furthermore, there were no statistically executive function improvement on follow-up in 4 studies with 138 patients (SMD = -0.30, 95% CI (-0.47, 0.24), p = 0.54, Fig. 6B), follow-up attention/working memory in 6 studies with 407 patients (SMD = -0.03, 95% CI (-0.24, 0.18), p = 0.78, Fig. 6C), follow-up memory in 5 studies with 387 patients (SMD = 0.13, 95% CI (-0.11, 0.37), p = 0.29, Fig. 6D) or follow-up language in 3 studies with 245 patients (SMD = 0.02, 95% CI (-0.27, 0.32), p = 0.88; Fig. 6E) either.
Effects of NIBS combined with CT in patients with different diagnosis on follow-upThree studies with 335 patients reported follow-up attention/working memory and follow-up memory scores in MCI. The pooled results showed that MCI did not achieved signifcant follow-up attention/working memory (SMD = -0.21, 95% CI (-0.44, 0.01), p = 0.06; Fig. 7A) or follow-up memory scores (SMD = 0.18, 95% CI (-0.04, 0.41), p = 0.11; Fig. 7B) improvement in NIBS combined with CT group.
Fig. 7
Meta-analysis of NIBS combined with CT in patients with different diagnosis on follow-up (A-C)
Six studies with 182 patients and 3 studies with 72 patients reported follow-up global cognition and follow-up attention/working memory in AD, respectively. The pooled results showed NIBS combined with CT signifcantly improved follow-up global cognition (SMD = 0.40, 95% CI (0.03, 0.77), p = 0.03; Fig. 7C) and follow-up attention/working memory (SMD = 0.72, 95% CI (0.23, 1.20), p = 0.004; Fig. 7D) in AD. However, 3 studies with 72 patients did not achieve signifcant follow-up language improvement in AD (SMD = 0.12, 95% CI (-0.37, 0.61), p = 0.63; Fig. 7E).
留言 (0)