
記住我




This study was conducted in strict adherence to national guidelines for ethical animal research and received approval from the local Institutional Ethics Committee on Animal Care and Use. Following overnight fasting, eight anesthetized and paralyzed pigs (mean body weight of 25 ± 1.0 kg) were mechanically ventilated using a MATRX VIP 3000™ Veterinary Anesthesia Vaporizer. Ventilation settings included an oxygen concentration (FiO2) of 35%, a tidal volume (TV) of 9 mL/kg, an inspiration/expiration ratio of 1/2, and a positive end-expiratory pressure (PEEP) of 7 cmH2O. The respiratory rate was adjusted to maintain arterial CO2 partial pressure (PaCO2) between 35 and 45 mmHg, and these settings were consistent throughout the experiment. For continuous monitoring of blood pressure and biochemical analyses, a catheter was inserted into the femoral artery. Hydration was maintained via intravenous administration of normal saline at a rate of 1.5 mL·kg^-1·h^-1 through a femoral vein catheter. The pigs remained supine throughout the study.
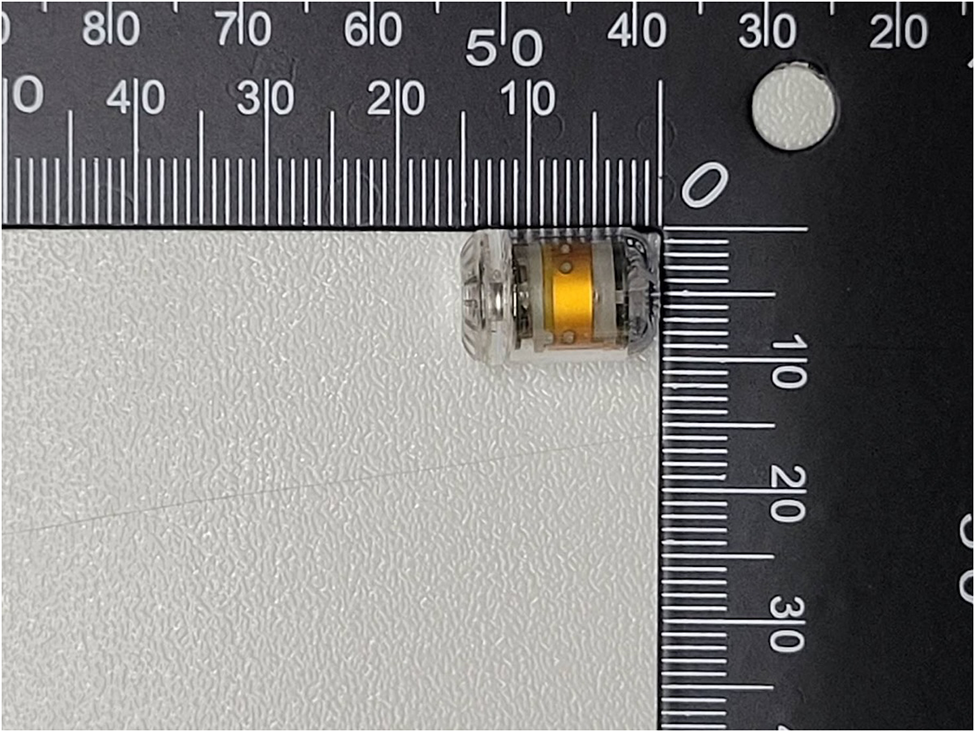
The animals were instrumented with three different IAP measurement devices. The capsular pressure sensors: PressureDOT (Dotspace Inc., Delaware, United states) (IAPdot, Fig. 1) were positioned transesophageal into the stomach.
Fig. 1
The swallowable capsular monitor device which used to detect intraabdominal pressure
The position was checked afterwards by radiography. (as Fig. 2)
Fig. 2
Radiographic imaging of a pig implanted with digital capsule for intraabdominal pressure monitoring
A small midline laparotomy was performed and a catheter (IAPdir) was placed intraperitoneally, caudally to the stomach. A Foley-based catheter with pressure transducer (IAPivp) was inserted into the bladder. The two catheters were exteriorized, and the laparotomy was carefully closed and water-sealed in two layers.
Measurements of IAPMeasurements of IAP were based on three different measurement principles.
PressureDOT capsular intraluminal IAP measurement (IAPdot)The measurement of intra-abdominal pressure was conducted using a commercial medical device, the PressureDOT (Dotspace Inc., Delaware, United states). This device is an ingestible capsule (12 mm in length and 6 mm in diameter) equipped with temperature and pressure sensors. The device’s accuracy is ± 0.5 °C for temperature and ± 0.5 mmHg for pressure. It has a battery life of 300 h and transmits data every 5 s via Bluetooth 5.0 to an external receiver connected to a laptop.
Intravesical pressure IAP measurement (IAPivp)Following bladder emptying under anesthesia, a latex catheter was inserted transurethrally and connected to a peristaltic pump for saline infusion. Pressure data were captured at 100 Hz using a PowerLab digital system (PowerLab 8/30, AD Instruments, Colorado Springs, CO), with the symphysis pubis serving as the zero-reference point for all measurements, regardless of the animal’s position [16].
Direct intraperitoneal IAP measurement IAPdirA multiple-hole catheter was placed intraperitoneally during a small midline laparotomy, positioned caudally to the stomach, and connected to a pressure transducer. Prior to measurements, the catheter was flushed with saline to ensure patency. The pressure transducer was also connected to the PowerLab digital system.
Experimental protocolThe pigs were positioned in a supine state to standardize the measurement setup. Initial baseline IAP was recorded to provide a reference for subsequent measurements. IAP was incrementally increased using a controlled infusion of carbon dioxide into the peritoneal cavity. Specific pressure targets set for the study were 10, 20, 30, and 40 mmHg. The actual pressure reached was verified using both the direct intraperitoneal catheter (IAPdir) and the barosensor connected to the inflator. At each target IAP level, there was a holding up period to permit the pressure to stabilize into a plateau. This stabilization period was crucial to ensure that the readings were consistent and reflective of a steady state. Following stabilization, IAP measurements were recorded continuously for 5 min to capture any fluctuations and to ensure the accuracy of the data. After recording at one IAP level, the pressure was gradually diminished to the following lower preset level or back to baseline. This stepwise decrease was carefully managed to avoid rapid changes that could affect physiological responses. Measurements were repeated at each level to assess the reproducibility and reliability of the data. After completing all planned observations and data recordings, the experiment was concluded with the humane euthanasia of the animals. This was carried out by first deepening the anesthesia to ensure no discomfort to the animals, followed by administering an additional dose of 4 mg of Pancuronium Bromide. Subsequently, euthanasia was achieved by injecting 60–100 mL of potassium chloride, effectively inducing cardiac arrest in a controlled and ethical manner.
Data acquisition and data analysisIntra-abdominal pressure measurements from the direct intraperitoneal catheter (IAPdir) and the intravesical catheter (IAPivp) were acquired using a multimodal monitor (PowerLab 8/30, AD Instruments, Colorado Springs, CO). This equipment was connected to a computer that enabled real-time data capture via a Local Area Network (LAN). Simultaneously, data from the PressureDOT device (IAPdot) were wirelessly transmitted to an external receiver and recorded onto a memory card at a frequency of 0.2 Hz via a serial port. To ensure the integrity of the data comparisons, the internal clocks of the three computers used for data acquisition were synchronized at the start of the data collection process. Subsequent to data acquisition, time-synchronized IAP readings from the various devices were analyzed offline using dedicated software (Excel, Microsoft Corporation, Seattle, USA). Each data set, referred to as a triplet, was recorded for individual animals, and pressure-time correlation graphs were generated to visually assess the dynamic changes in IAP.
Given the continuous nature of the data collection, we were able to perform detailed comparative analyses between the different IAP measurement modalities for each subject. Summarized data across all subjects were aggregated according to IAPdir levels, facilitating a comprehensive comparison of correlations between IAPdot, IAPivp, and IAPdir. The IAPdir measurement was considered the reference standard, representing the true pressure within the abdominal cavity. Disparities between the measurements obtained from IAPdot and IAPivp relative to IAPdir were methodically analyzed at set pressure increments of 5, 10, 15, 20, and 30 mmHg. All intra-abdominal pressure values were uniformly expressed in millimeters of mercury (mmHg), standardizing the data for analysis and reporting.
Statistical analysisResults are reported as mean ± standard deviation (SD) to quantify the variability and central tendency of the data. The degree of linear correlation between the different intra-abdominal pressure (IAP) measurement methods was evaluated using Pearson correlation coefficients, and the strength of this association was further quantified by calculating the coefficient of determination (R² values). Statistical significance was assessed using a two-tailed t-test, with a p-value of less than 0.05 considered to indicate statistically significant differences between measurement methods.
留言 (0)