
記住我









This retrospective study was conducted between August 2013 and October 2023 in the department of Obstetrics and Gynecology of Chungnam National University Hospital and Chungnam National University Sejong Hospital, which are tertiary referral centers for high-risk pregnancies. This study was approved by the Ethics Committee of Chungnam National University Sejong Hospital (IRP No. 2023-12-004). PPH was defined as blood loss exceeding 500 mL, regardless of the mode of delivery (vaginal or cesarean section), according to the WHO definition of PPH. Cases of primary PPH occurring within 24 h of delivery and secondary PPH occurring between 24 h and 12 weeks after delivery were included.
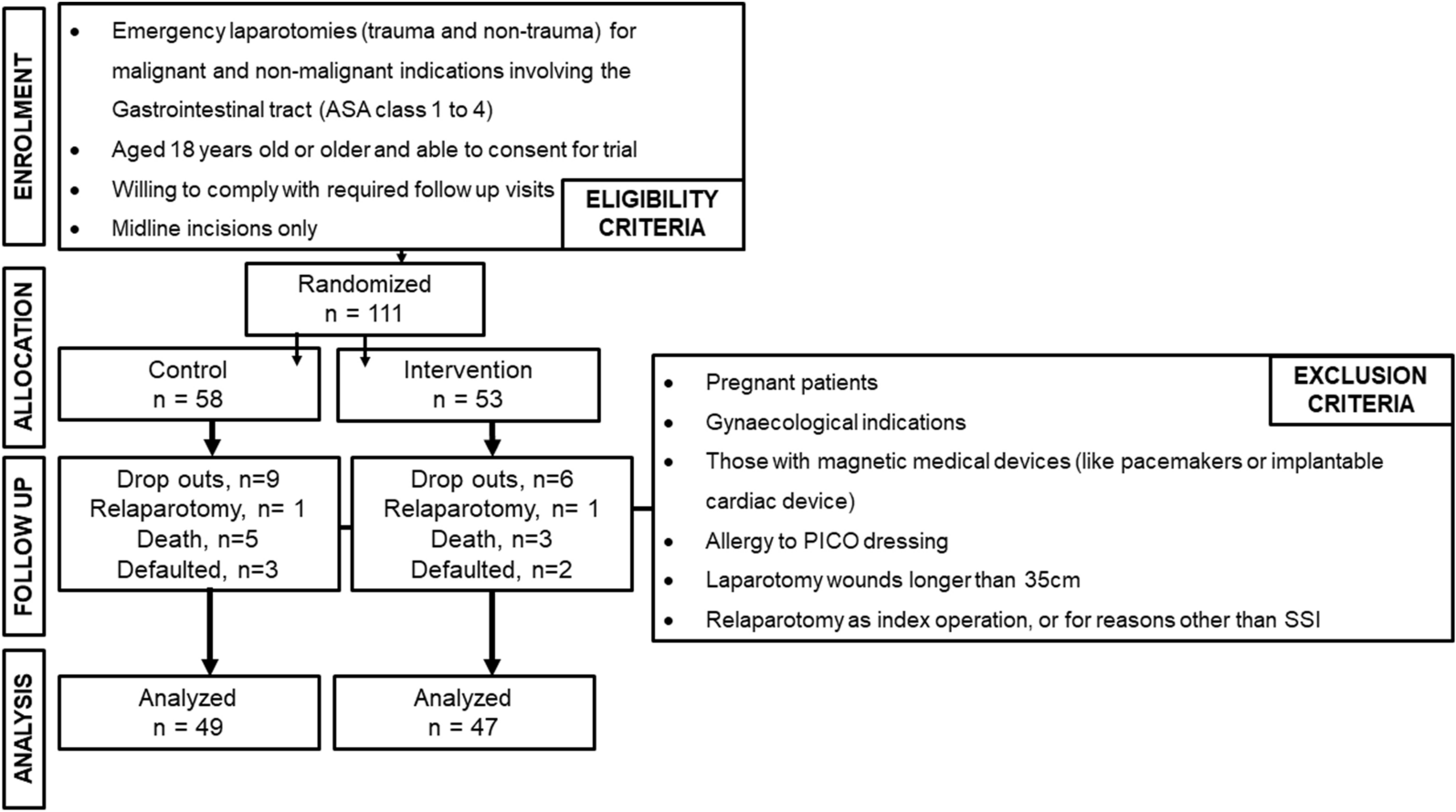
Figure 1 shows the selection of the participants. Women diagnosed with PPH were included in the study. Of the 272 recruited patients, 42 were excluded because their estimated blood loss (EBL) was less than 500 mL, or no blood transfusion was performed. The remaining 230 patients were divided into two groups: non-surgical intervention (group 1, n = 159) and surgical intervention (group 2, n = 71). The surgical intervention group was further divided into two groups for subgroup analysis: immediate surgical intervention (n = 45) and delayed surgical intervention after the failure of non-surgical intervention (n = 26). First-line treatments included uterotonics, hemostasis, uterine massage, manual removal of residual placental tissue, gauze packing, and bimanual compression maneuvers. Second-line treatments included BBT and UAE. Surgical interventions included B-Lynch suturing, uterine artery ligation, surgical bleeding control or laceration repair, surgical placental removal, and hysterectomy. Failure of non-surgical intervention refers to the failure of second-line treatment.
Fig. 1
Flowchart of the study participant selection. EBL = estimated blood loss, BBT = Bakri balloon tamponade, UAE = uterine arterial embolization
The decision to perform surgery was made according to the institutional criteria. When patients with PPH visited the hospital, only first-line treatment was administered if their vital signs were stable, EBL was less than 1 L, or vaginal bleeding required 1–2 pads/h. If the EBL was 1–2 L or more than 2 pads/h, the second-line treatment was administered simultaneously with the first-line treatment. Surgery was performed immediately if the EBL exceeded 2 L and there was clinically severe and persistent uncontrollable hemorrhage or unstable vital signs.
The baseline obstetric characteristics of women with PPH, such as age, body mass index (BMI), parity, singleton or multiple pregnancies, gestational age at delivery, type of delivery (vaginal delivery vs. cesarean section), delivery location (inborn vs. outborn), baby weight, and previous uterine surgery (including a history of cesarean section or myomectomy), were obtained from the records. The time of PPH onset (< 24 h after delivery, or > 24 h after delivery up to 12 weeks), initial laboratory information, and initial vital signs were obtained from the records. Initial laboratory tests included white blood cell (WBC) count, hemoglobin, hematocrit (Hct), platelets, and lactic acid level. The initial vital signs included systolic blood pressure (BP), diastolic BP, heart rate, body temperature, and shock index (SI). The SI was calculated as heart rate divided by systolic BP.
The causes of PPH were classified according to the 4 Ts. “Tone” includes uterine atony, and “trauma” includes uterine wall rupture and genital tract injury. “Tissue” includes retained placenta and clots and abnormal placentation. “Thrombin” includes placental abruption, pre-eclampsia, and coagulation abnormalities. Abnormal placentation includes placenta previa and placenta accreta syndrome; genital tract injuries, including perineal, cervical, and vaginal lacerations; and extrauterine bleeding, including bleeding in the abdominal wall, intraperitoneal cavity, and surrounding organs.
Data on PPH and morbidity outcomes were also analyzed. The survey items were total EBL, total number of blood transfusion packs, mean hospital stay, intensive care unit (ICU) admission rate, mortality, and complications. Total EBL was estimated by measuring the weight of the blood-soaked pad, the weight of the gauze used before and after the procedure, and the amount of blood contained in the irrigation bottle used during surgery. One milliliter of blood, weighing approximately 1 g, was used. Blood transfusions were calculated as the number of red blood cell (RBC), fresh frozen plasma (FFP), and platelet transfusion packs. Complications included disseminated intravascular coagulopathy (DIC), fever, hypertension, wound infection, acute renal failure (ARF), pulmonary complications such as pulmonary edema and pulmonary effusion, cardiac complications such as heart failure and arrhythmia, cerebral complications such as cerebral hemorrhage, stroke, and headache, deep vein thrombosis (DVT), and Sheehan syndrome. In the subgroup analysis, we further investigated the following outcomes: time from decision to transfer to the start of surgery, hysterectomy rates, and surgical complications, including bladder injury, ureteral injury, and intestinal complications.
Statistical analysisQuantitative variables were described as mean ± standard deviation. Qualitative variables were described as frequencies (n) and proportions (%). An independent-samples t-test was used to compare the two groups. Logistic regression analysis was performed on the variables that showed significant differences in the t-test. Statistical significance was defined as a p-value < 0.05. The statistical program SPSS (IBM SPSS Version 22.0) was used for analysis.
留言 (0)