Missed and delayed diagnosed injuries (DDI) have been shown to affect trauma patients’ morbidity and mortality [2, 3]. Understanding of the underlying etiology is crucial for minimising incidence rate in multiply injured patients. Furthermore, identifying circumstances in which DDI are more likely to occur helps to raise suspicion in the treating trauma team.
To investigate undetected injuries, it is of pivotal importance to first consent a definition of missed and delayed diagnosed injuries.
Missed injuries (MI) refer to injuries that have not been detected throughout the entire in-hospital treatment. In contrast, delayed diagnosed injuries (DDI) have been detected during hospital stay, but delayed, meaning not at the time they could have been detected. DDI may therefore impact treatment during initial hospital stay. During primary survey in the ED the emergency team needs to identify life-threatening injuries first. During secondary survey, all injuries should be identified through a thorough examination by the trauma team with high suspicion. In this study, injuries first diagnosed in ICU are defined as ‘delayed diagnosed injuries’.
Incidence of DDI
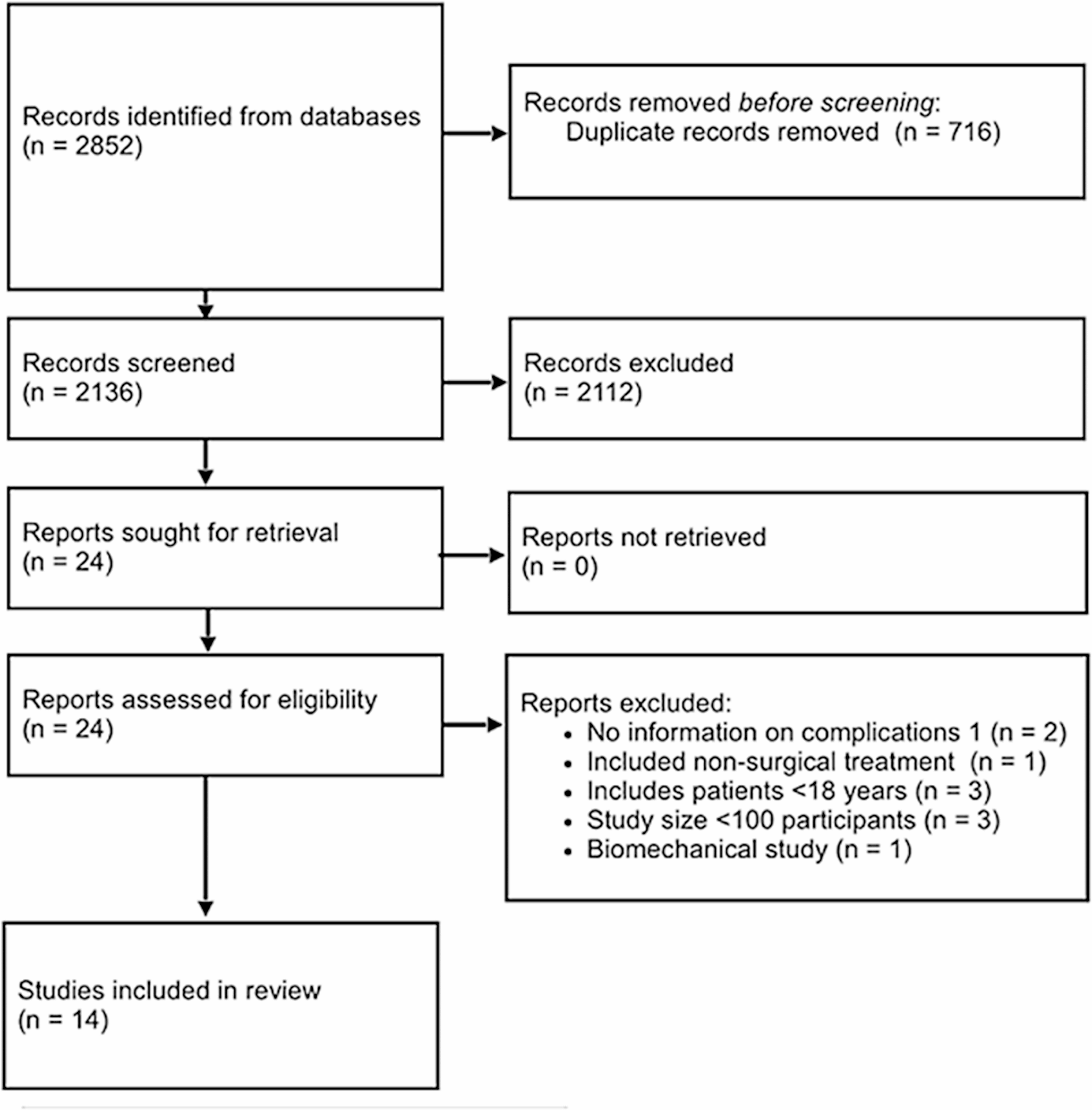
In this study, delayed-diagnosed injuries (DDI) were evaluated in the largest cohort of multiple trauma patients. DDI occurred in 9.2% of patients. 35.8% of delayed-diagnosed head injuries, 19.7% of thoracic injuries, and 33.3% of extremity injuries were found. 11.1% had abdominal, and 9.4% had delayed-diagnosed spine injuries.
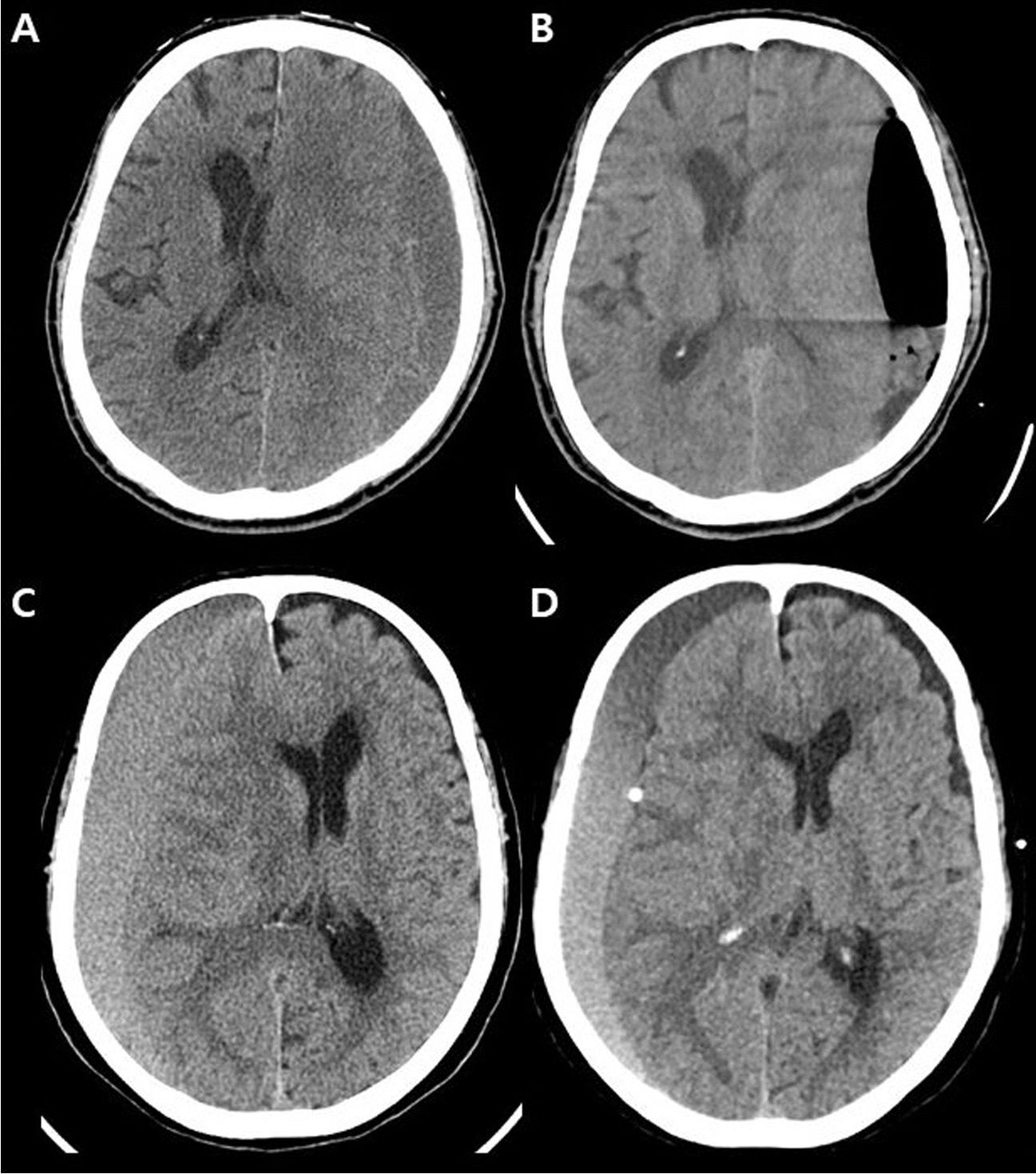
Published incidence rates of DDI vary largely in the literature depending on the definition and study cohort. Incidence rates from 1.3% up to 25.8% have been reported in studies with limited sample sizes [2,3,4,5, 19,20,21,22,23]. In 1991, Laasonen et al. investigated missed injuries in 340 patients and identified 8.5% of these patients [21]. Similar results have been published by Buduhan et al. in 2000. The study group reports that 8.1% of 567 patients have missed injuries [2]. Vles et al. found missed injuries in only 1.3% of 3,879 patients in a prospective study published in 2003 [19]. In contrast, Brooks et al. published one year later, in 2004, a delayed injury rate of 22.2% in severely injured patients [3]. In 2011, Lawson et al. published an incidence rate of 9% in a larger cohort of 26,264 patients. This incidence rate is in line with our results. Reasons for differences in reported rates of MI and DDI beside unequal definitions and study cohorts are improving standards and procedures in the ED. They have contributed to reduce the rate of DDI over the last decades. For example, multislice computed tomography (MSCT), which is now a standard diagnostic modality in polytrauma patients, was not available to this extent 20 years ago. Also, implementation of standard course formats like ATLS® and emergency room trainings might have improved skills and expertise among trauma doctors worldwide [24]. The relatively high number of patients with delayed diagnosed head injuries raises the question of whether routine follow-up CT scans, especially in unconscious patients, may close a diagnostic gap since subdural hematomas may develop within 24 h to 48 h after trauma. Furthermore, following a high-energy trauma abdominal CT scan after 12 h to 24 h hours may reveal bowel or splenic injury that remained undetected on initial CT scans even when reviewed retrospectively.
Also, available tools like artificial intelligence (AI) may help to reduce DDI rates [25].
Finally, one has to keep in mind that a certain number of lesions (e.g., cerebral edema) may develop during the clinical course. Therefore, they might be diagnosed after the initial workup, leading to a misdocumentation as DDI. In a registry, those diagnoses cannot be identified reliably ex post.
Finally, one has to consider that some lesions addressed as DDI might also result from early interventions during initial treatment. For example, a pneumothorax might be caused by introducing a central venous line to the vena subclavia. Those entities are not to be identified by registry records.
As stated initially, the trauma team’s experience plays an important role in treating severely injured patients. Although individual training of team members is mandatory, monitored team performance depends on team training. Given a greater number of severely injured patients, teams in level I trauma centres may have more training, and management includes the identification of frequently missed injuries. This may also apply for ICU staff and may have led to a higher proportion of patients with DDI treated in level-2 and 3 hospitals.
How different hospital levels and patient numbers can affect the incidence of DDI and how this can be improved, i.e. team training, should be subject to further analysis.
Factors influencing DDI
While treating multiple injured patients in the ED, the reported mechanism of injury gives valuable information on associated injuries. In car accidents, injuries to the thorax and lower extremities are frequently observed. In contrast, patients sustaining a fall from a height greater than 3 m have a higher chance of sustaining injuries to the lower extremities and spine [26, 27].
Overall, patients with DDI were more likely to be hypotensive at initial presentation (12.6% vs. 18.7%), showed a higher transfusion rate (8.7% vs. 15.7) and were more likely to be unconscious (17.0% vs. 25.1%). Due to the higher injury severity in DDI patients (ISS 25.0 versus 18.5), emergency surgery was significantly more often performed in patients with DDI (29.3% vs. 23.5%). Head injuries were much more prevalent in DDI cases. However, in some of these cases, intra-cranial bleeding may have progressed so that these injuries were not apparent in the initial scans. We did not find a correlation between age and incidence of DDI.
Possibly, DDIs occur due to a prioritised intervention in the ED before finishing a proper secondary survey following the paradigm ‘Treat first what kills first’. Undetected injuries may arise since resuscitation of severely injured patients has priority over complete identification of all injuries, especially in patients ‘in extremis’. Doing so, minor injuries might be identified during the ‘tertiary survey’ after resuscitation in the ICU. Even injuries that develop with latency contribute to a higher number of DDI.
The concept of a tertiary survey within 24 h has been shown to reduce the incidence of DDI [28]. The tertiary survey is a complete and systematic patient reevaluation, including primary and secondary surveys and a review of radiographs usually performed in the ICU after initial resuscitation. However, in a prospective study by Keijzers et al. evaluating a formalised tertiary survey, the authors did not find a significant reduction of missed injuries. Still, they reported a high number of injuries not detected within the initial hospital stay. Especially in patients with neurologic compromise, clinical examination can be challenging.
Finally, the value of the initial radiological workup needs to be discussed.
However, in advance, we have demonstrated that initial whole-body computed tomography is highly specific but has variable sensitivity for the detection of injuries in patients with suspected blunt trauma. In this context, we found that the best balance between sensitivity and specificity was achieved when the WBCT was performed about 30 min after admission [20].
The Risk for Delayed Diagnoses Score (RIDD-Score)
Within the presented study we were able to figure out a score estimating the risk of a DDI of an individual patient. This simple to be used instrument helps identify patients under risk already at the very beginning of the initial emergency treatment. However, in reverse, this does not mean that patients with a low score should be managed less thoroughly initially (Fig. 3).
Limitations
Several factors may limit the results of this study and must be interpreted carefully. In addition to a possible selection error, register data are generally less valid than data provided by prospective randomized controlled studies.
Furthermore, DDI are defined as injuries first observed on ICU as diagnoses of patients in the TraumaRegister DGU® can only be differentiated between injuries identified in the ED and injuries first diagnosed on ICU. Furthermore, injuries missed until discharge from the hospital are not documented. The time point of diagnosis was not documented in all cases, and assumably, not all DDI were documented in the TraumaRegister DGU® as it requires active marking in the web-based interface.
Also, diagnoses in the TraumaRegister DGU® are documented as AIS codes. This may limit accuracy of delayed diagnoses as no exact code exists for each injury type.
Further studies need to investigate outcome of delayed diagnosed injuries.

留言 (0)