Design
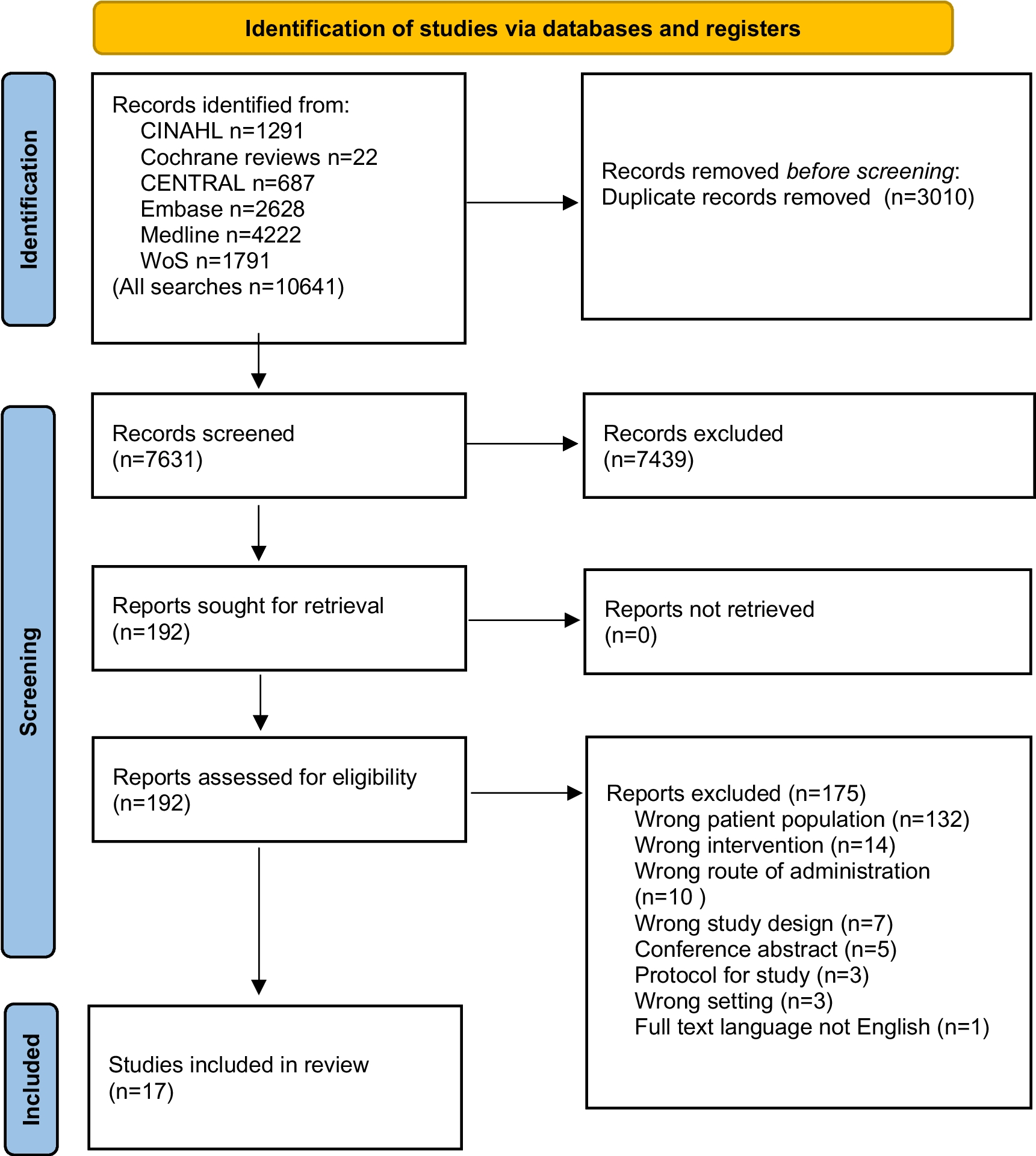
The data for this analysis are from the PANUSCO trial (NCT01362582). PANUSCO was a controlled, open-label, prospective, randomized, phase IIIb, multicenter trial with two parallel arms to investigate the effects of PN (intervention group (IG)) in combination with BSNC versus BSNC alone, (control group (CG)) on event-free survival in patients with advanced PaCa [40] (Fig S I).
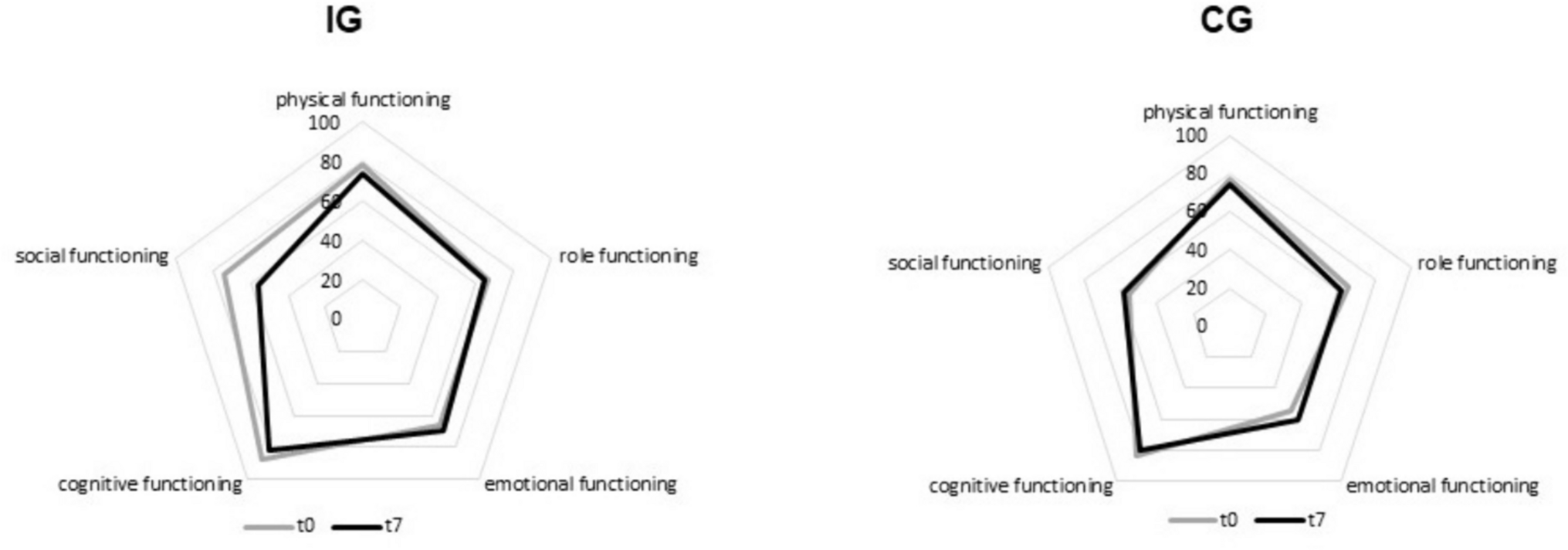
The study was terminated prematurely because the calculated sample size of 120 patients could not be achieved. In this secondary analysis, the available datasets from four centers (Heidelberg, Erlangen, Bad Soden, Greifswald—Germany) were evaluated in an exploratory way. Data sets from weekly visits from baseline (t0) to week 7 (t7) were analyzed (our baseline represents t1 of the study protocol). The primary endpoint of this exploratory analysis was the change of QoL over 7 weeks between groups. Furthermore, correlations between changes in EI as well as protein intake (PI) and changes of QoL were investigated for all participants irrespective of group allocation.
Participants
Patients over 18 years of age with histologically confirmed advanced pancreatic adenocarcinoma who had received at least one prior CTx (gemcitabine-based) and experienced disease progression on this prior CTx were screened for participation. At enrolment, all patients received 5-fluorouracil (5-FU), folinic acid (FA), and oxaliplatin as second or higher line CTx [40]. QoL-related inclusion criteria were a body mass index (BMI) ≥ 19 kg/m2, an expected life expectancy of more than 3 months, and at least one previous CTx. QoL-related exclusion criteria were a major surgery of less than 4 weeks prior to enrolment, a WL of more than two percentage within the last 7 days or an EI less than 500 kcal expected within the next 5 days, and more than 4 weeks of PN within the last 6 months or PN less than 4 weeks prior to enrolment. Detailed inclusion and exclusion criteria are given in [40]. Patients were randomly assigned to IG or CG.
Nutrition of the patients
Both, the IG and CG received BSNC, defined as weekly nutritional consultation (face-to-face or by phone) and recommendation by experienced nutritionists. All types of oral nutritional supplements were allowed. Independent of oral food intake, the IG additionally received a defined, supportive PN. Defined stop criteria for nutritional therapy, e.g., energy intake of at least 50% of requirements, ensured that an adequate supply of nutrients was guaranteed for both the CG and IG. The infusions contained 1150 kcal, 50 g amino acids, 125 g glucose, and 38 g (+ 5 g fish oil extra) fat with soybean oil, medium chain triglycerides, olive oil, and fish oil. PN was planned to be given continuously overnight, 6 days per week at home. The actual administration of PN was recorded. The parentally prescribed EI was the same for all participants and did not depend on body weight (BW) or NS. This was not a total PN, but supplemental PN for all. Detailed information of PN is described in [40].
The NI as well as the CTx was administered until individual discontinuation criteria were met. For both arms, there were individual stopping criteria for the NI (Tab S I).
Quality of life
The European Organization for Research and Treatment of Cancer (EORTC) quality of life questionnaire (QLQ-C30) and its supplementary module for PaCa QLQ-PAN26 in the validated German translation were used for assessing health-related QoL. A scoping review showed that the QLQ-C30 questionnaire was the most commonly used disease-specific instrument for QoL assessment in patients with PN and EN [41]. The QLQ-C30 with 30 questions is composed of both multi-item scales and single-item measures [42]. The questionnaire consists of five functional scales (physical, role, emotional, cognitive, and social functioning), three symptom scales (fatigue, nausea/vomiting, and pain), a global health status/ QoL scale, and six single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties) [42]. The domain role functioning asks if there were any limitations during work or leisure. The QLQ-PAN 26 includes 26 questions. It consists of seven scales, five of which are symptom scales (pancreatic pain, digestive symptoms, altered bowel habit, hepatic symptoms, and body image) and two functional scales (satisfaction with health care and sexuality). In addition, 10 single items are surveyed (symptom items: bloating, taste, indigestion, flatulence, WL, weakness arms and legs, dry mouth, trouble with side effects, future worries, and planning of activities). The scale of digestive symptoms asks whether there were any limitations in food selection and quantity due to the disease or treatment. The item WL asks if patients are concerned about low BW. There are four answer options (not at all, a little, quite a bit, very much) for each question in both questionnaires. All scales and single items are transformed to a scale from 0 to 100 [42]. A high score in the functional scale represents a high/healthy level of functioning [42]. A high score in global health status/QoL represents a high QoL [42]. However, a high score in symptom scale/item represents a high level of symptomatology/problems [42]. The different domains of the QLQ-C30 and QLQ-PAN26 were evaluated separately.
Sample size
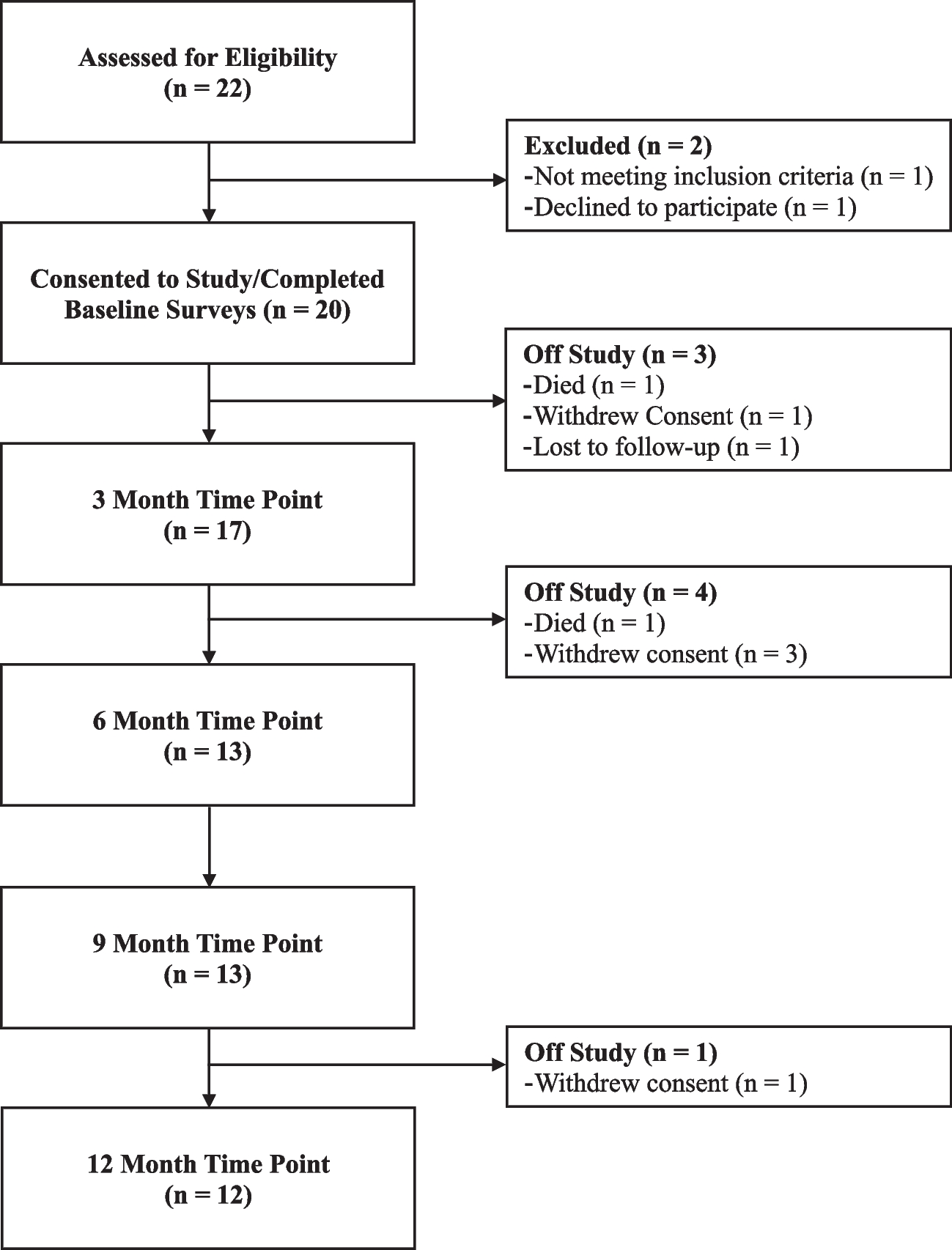
A total of 31 patients were enrolled in PANUSCO at four centers, and data on QoL were available for 30 patients. Data from patients who participated in the study for at least 7 weeks were analyzed. Therefore, 21 patients (IG: n = 9; CG: n = 12) were included in this secondary analysis.
After the patient’s eligibility for randomization was assessed, patients were randomly assigned to one of the two treatment arms (1:1) Stratification was performed prior to randomization by Eastern Cooperative Oncology Group Performance Status (ECOG PS) (stratum 1: PS < 2, stratum 2: PS ≥ 2) [40].
Statistical analysis
Descriptive statistics (means and standard deviations) were performed for patient characteristics and for all items of QLQ-C30 and QLQ-PAN26. For missing data of patient characteristics, the last available data were imputed. For single missing items of QLQ-C30 and PAN26, they were rated as missing, as recommended in the EORTC manual [42]. However, only one item of one patient in the QLQ C30 questionnaire was missing. In QLQ-PAN26, two items were missing in four patients. These included questions on sexuality, which, according to the manual, can often lead to problems with the questionnaire [42]. The data set did not meet the requirement for parametric statistical procedures. Therefore, Wilcoxon tests were performed for all items of QLQ-C30 and QLQ-PAN26 for each group to test for changes over the course of the 7-week intervention. Mann–Whitney U-Tests were performed for all items of QLQ-C30 and QLQ-PAN26 to test for differences between the groups at baseline (t0), at the end of the analysis period (t7), and for change from t0 to t7 (delta). Spearman’s rank correlation test was performed to test the correlation between the changes of all items of (a) QLQ-C30 and (b) QLQ-PAN26 with the changes in PI in g/kg BW, the changes in EI, and the changes in BW from t0 to t7 for all participants irrespective of group allocation. All tests were performed with exact significance and were two-tailed. p < 0.05 indicates statistical significance. The IBM SPSS version 28.0 software, Chicago, IL, USA, was used.



留言 (0)