The use of OAs in cancer patients receiving ICI therapy has become a topic of increasing interest and discussion within the oncology field. This study aims to explore the impact of OAs on survival outcomes in cancer patients undergoing ICI treatment, with a focus on balancing effective pain management and potential immunomodulatory consequences. DDIs have gathered significant attention in the context of identifying patients who benefit from ICI therapy more and who have durable benefits. OAs constitute a significant component of the medications routinely given to cancer patients. Nevertheless, the potential effects of opioids on interactions with ICIs and their role in relieving cancer-related pain are not yet fully comprehended.
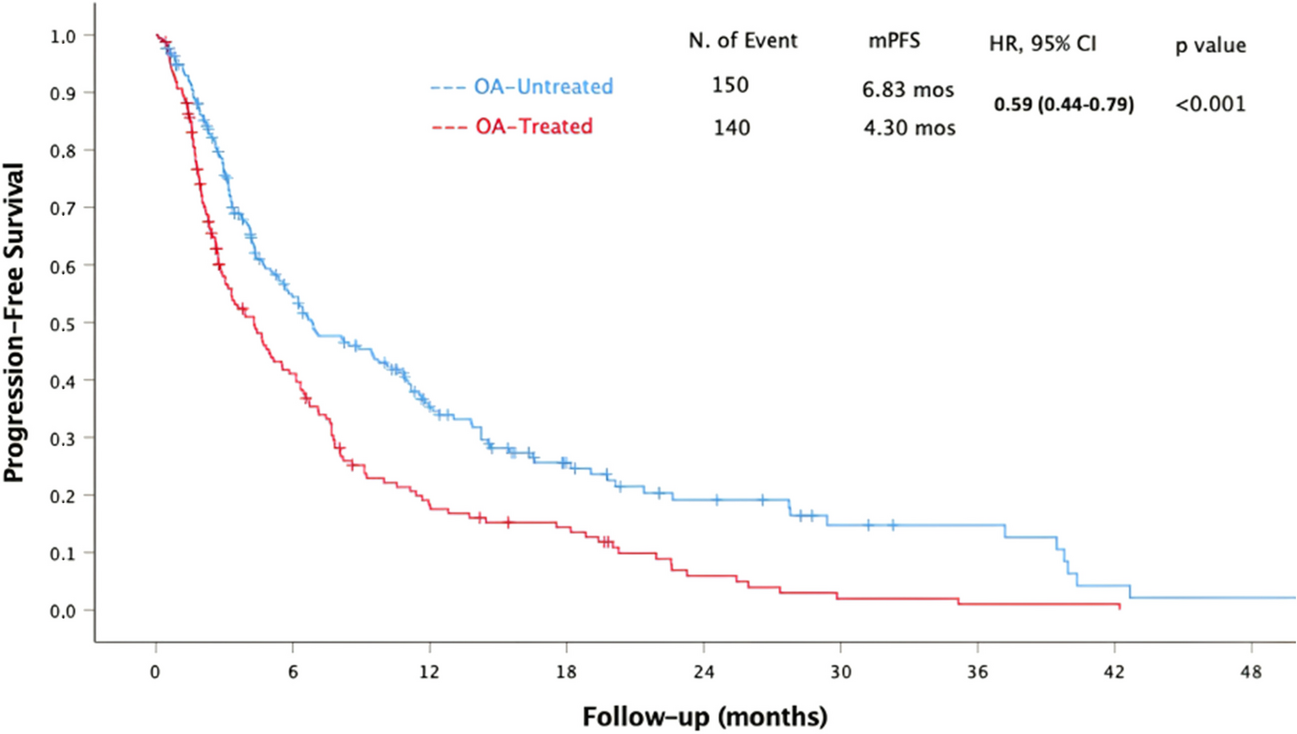
Our findings reveal a noteworthy association between OA treatment and significantly reduced PFS and OS in cancer patients receiving ICI therapy. Consistent with previous research hinting at the potential negative influence of opioids, our results highlight that the impact of opioids varies by tumor type, suggesting a need for tumor-specific strategies in clinical practice [6,7,8,9]. The relationship between an ECOG PS of 1 or higher and reduced OS, elevated LDH levels above the normal range, and reduced PFS and OS suggests an association between increasing disease burden and OA usage, which may be related to a worse prognosis. Additionally, patients using OA had a higher number of previous treatment regimens, possibly due to underlying factors related to increased disease burden, and this could contribute to decreased survival. This association was particularly noted in malignant melanoma and NSCLC. However, the absence of a similar relationship in RCC and other tumors indicates the potential involvement of different underlying mechanisms. It is also important to consider that the smaller number of patients in other tumor types may impact the interpretation of these results.
Mechanistically, OAs like morphine can impact cancer progression via various pathways. OAs often employed for severe pain management through the activation of the mu (μ) opioid receptors [10] might impact cancer patients’ outcomes during ICI treatment as μ-opioid receptor is also expressed in the cells of the immune system, such as lymphocytes and macrophages [11]. Preclinical investigations have uncovered that opioids such as morphine can trigger tumor proliferation, suppress apoptosis, enhance angiogenesis, and facilitate the invasion of cancer cells through various mechanisms, including EGFR phosphorylation in lung cancer [12], activation of the MAPK/ERK pathway in endothelial cells in breast cancer [13], and induction of urokinase plasminogen activator secretion in colon cancer [5]. Moreover, ICIs’ efficacy depends on anticancer immunity, and opioids may contribute to an immunosuppressive tumor microenvironment. Morphine has been shown to inhibit the transcription of IL-2, a critical cytokine for CD8 + T cell activation, and increase cAMP levels, impairing T-cell receptor signaling and CD8 + T cell function [14]. Additionally, opioids can downregulate major histocompatibility complex class II expression in antigen-presenting cells, inhibiting CD4 + T cell activation and cytokine secretion [15]. Furthermore, opioids can lead to an increase in regulatory Tregs, further hindering the anticancer immune response [16].
Another crucial aspect is the connection between gut dysbiosis and ICI efficacy as imbalances in the gut microbiota can reduce a patient’s response to ICIs [17]. Long-term opioid use, which often results in gastrointestinal side effects, may exacerbate this issue [18]. Opioids can suppress protective mucus and bicarbonate secretion from the intestinal epithelium, weaken myenteric activity, and potentially raise the risk of bacterial translocation [18, 19]. Morphine, in particular, has been found to damage the intestinal epithelial integrity and alter the gut microbiota composition, favoring pathogenic bacteria [18, 20]. These complex interactions underscore the importance of considering the impact of opioids on cancer patients undergoing ICI therapy, urging further research in this field.
Our study, being retrospective in nature, comes with several inherent limitations. It includes a heterogeneous population with variations in primary tumor types, treatment lines, and the types of ICIs administered. Additionally, the OA treatment is more common among patients with high tumor burden and associated symptoms, all of which could potentially act as confounding factors in our retrospective analysis. It was challenging to assess the impact of each specific opioid on survival, as many patients underwent opioid switching during their immunotherapy, often involving different dosages. To address these limitations, future prospective studies should involve larger and more homogeneous patient cohorts while collecting detailed data on opioid dosages, types, and duration of use to validate and expand upon our findings.
Our study provides valuable guidance for oncologists in their clinical practice. It is important to recognize that OAs play an important role in managing cancer-related pain and improving the quality of life for many patients. The decision to prescribe opioids should always be individualized, taking into account the patient’s level of pain, the risk of addiction, and now, the potential impact on cancer outcomes when used with ICIs. To optimize patient outcomes, it is critical to incorporate evidence-based guidelines into clinical practice. Multimodal analgesia, which combines different classes of analgesics and nonpharmacologic interventions, should be prioritized to minimize opioid use and mitigate potential adverse effects. Clinicians should explore alternative pain management strategies, including non-opioid analgesics or interventional procedures, whenever appropriate. Non-opioid analgesics, such as acetaminophen and NSAIDs, should be considered first-line options for mild to moderate pain [21]. For severe pain, adjunctive therapies such as nerve blocks, epidural analgesia, and neuromodulation techniques can provide effective pain relief while reducing the need for opioids [22]. In addition, early integration of palliative care into the treatment continuum has been shown to improve both quality of life and survival outcomes for cancer patients [23]. Palliative care teams can provide comprehensive pain management strategies and psychosocial support to achieve better pain control without relying solely on opioids. Education and training programs for healthcare providers on safe opioid prescribing practices and management of opioid-related side effects are also essential to ensure the safe and effective use of OAs in cancer pain management [24].
In conclusion, the delicate balance between effective pain management and the efficacy of cancer immunotherapy poses a challenging clinical dilemma. Our study provides valuable insights into the potential adverse effects of OAs on survival outcomes in cancer patients undergoing ICI therapy. Clinicians must carefully weigh the benefits of pain relief against the possible negative impact on the immune response and cancer outcomes when considering the use of opioids in this patient population. These findings do not imply the discontinuation of opioid use in cancer patients, as the need for opioids in advanced cancer patients with severe pain is crucial for improving their quality of life. We believe that the primary factor contributing to reduced survival is the high disease burden, but there may also be some additional immunological factors at play, especially considering that we could not observe this relationship in patients with RCC. However, it is essential to emphasize the importance of maintaining this balance. Further research is warranted to better understand the underlying mechanisms and refine clinical guidelines for pain management in cancer patients receiving immunotherapy.



留言 (0)